
Updates to CMS CoP Interpretive Guidelines: Discharge Planning Evaluation & Choice Process
The interpretive guidelines emphasize that hospitals must assess each patient’s likely need for healthcare, non-healthcare, and community-based services following discharge.
By Tiffany Ferguson, LMSW, CMAC, ACM
In a recent article, I focused on the screening and discharge planning policy requirements for §482.43 Discharge Planning found in the Centers for Medicare & Medicaid Services (CMS) Conditions of Participation (CoP) Interpretive Guidelines, The State Operations Manual (SOM), Appendix A. This article will cover the most important aspects of case management practice: the discharge planning evaluation (i.e. initial assessment) and the choice process.
The interpretive guidelines emphasize that hospitals must assess each patient’s likely need for healthcare, non-healthcare, and community-based services following discharge. This expectation applies to all patients who have been screened or consulted, regardless of whether their anticipated trajectory is straightforward or complex.
Healthcare services may include the following:
Home health, personal attendant care, and/or other community-based services;
Hospice or palliative care;
Respiratory therapy;
Rehab services (physical, occupational, speech) and/or post-acute placement;
End-stage renal disease dialysis services;
Pharmaceuticals and supplies;
Substance use or behavioral health treatment;
Nutritional consultation and supplemental supplies; and
Durable medical equipment (DME).
At the same time, CMS has expanded the definition of essential post-discharge services to encompass non-traditional supports that directly affect the patient’s ability to remain in the community.
These may involve the following:
Home modifications or safety improvements;
Transportation assistance;
Meal delivery or nutrition programs; (and)
Household services such as shopping or housekeeping.
Once the needs are identified, hospitals are required to determine whether services are available and accessible in the patient’s community. This requires that case management programs maintain current knowledge of local providers, including not only skilled nursing facilities (SNFs) and home health agencies (HHAs) but also behavioral health providers, dialysis centers, equipment suppliers, and community-based organizations.
A key expectation in the guidelines is that hospitals cannot simply recommend services; they must ensure that those services are realistically obtainable by the patient. Accessibility includes consideration of insurance coverage, transportation to appointments, language or cultural barriers, and the patient’s ability to participate in care. If the patient or their informal caregivers cannot independently meet the required needs, the evaluation must determine whether community-based alternatives exist that allow the patient to remain at home, rather than defaulting to institutional placement.
Another critical component is coordination with insurers, including Medicare Advantage (MA) and Medicaid plans. Hospitals are required to verify that prescribed services are approved, covered, and available, to prevent scenarios in which patients are discharged with care plans that cannot be implemented. This payer coordination ensures not only compliance, but also practical feasibility of the discharge plan.
The ongoing documentation must demonstrate the arrangement of the discharge plan. This includes the following:
Educating patients and caregivers on self-care responsibilities;
Providing training to family or support people who will assist post-discharge;
Coordinating transfers to post-acute/rehabilitation or long-term care facilities when needed;
Making referrals to home health, hospice, behavioral health providers, etc.; and
Facilitating access to medical equipment and community support.
The process must also ensure that patients are given clear instructions on how to handle issues after discharge, including whom to contact with concerns, when to follow up with providers, and what symptoms or circumstances should prompt urgent or emergency care.
CMS emphasizes that the process is collaborative and must include the patient, their representative, and/or other family or informal caregivers who will provide care at home. Patients and caregivers must be kept informed throughout plan development and be provided with education and training tailored to their roles. Evidence of this collaboration must be documented in the medical record.
The guidance cautions hospitals against directing patients toward specific providers, instead emphasizing the freedom of choice among Medicare-participating post-acute facilities or agencies. When patient preferences cannot be accommodated, such as when a preferred SNF has no available beds, hospitals must document the reason and communicate transparently with the patient or representative.
As seen by hospitals, the guidance was clear that referrals cannot be blanketed to post-acute facilities, without confirming with the patient that those specialized services are required and that the patient consents to those services first. Similar to other processes, CMS emphasizes patient autonomy, collaboration, and inclusion in the process.
The plan must reflect their actual needs.
Some of the questions included in the guidelines include, among others, the following:
Does the evaluation identify both healthcare and community-based service needs?
Does the hospital demonstrate knowledge of available providers and services in its service area?
Is there evidence in the medical record of how the evaluation informed the discharge plan?
Was the plan discussed with the patient and/or representative, with documentation of that discussion?
Were patients provided with lists of Medicare-participating providers, when applicable, along with disclosure of any financial interests and inclusion of data on quality ratings?
The expanded requirements for discharge planning evaluations reflect the CMS recognition that safe transitions depend on comprehensive, realistic, and patient-centered planning. For hospitals, compliance will require interdisciplinary collaboration, robust knowledge of community resources, and an understanding of payer networks.

Prepare for Aetna to change inpatient payment policy in november
While the policy aims to streamline approvals and reduce outright denials, it raises substantial compliance questions under CMS regulations regarding medical necessity determinations, appeal rights, and contractual payment terms.
By Eileen Sullivan, MSN, CMAC, CCM, ACM-RN
Effective November 15, 2025, Aetna will implement a new Level of Severity Inpatient Payment Policy for Medicare Advantage (MA) and Medicare Special Needs Plan (SNP) members.
Key Points:
Automatic Approval: Urgent and emergent inpatient admissions will be automatically approved for MA/SNP members.
Payment Determination: Admissions that do not meet MCG inpatient criteria will still be approved as inpatient but reimbursed at a lower-severity inpatient rate, not outpatient or observation.
Reimbursement: These cases will be paid as inpatient (IP) downgrades, similar in concept to DRG downgrades.
No Denials: These are not considered medical necessity denials; therefore, no member or provider appeal rights are triggered under denial protocols.
Provider Notification:
Hospitals will receive concurrent notification of downgrades.
A physician-to-physician “discussion” will be available during the concurrent review process (not labeled as peer-to-peer/denial-related).
No Member Impact: MA members will not be notified of the downgrade, and their cost-sharing/copayment will not be affected.
Observation Status: These cases are not reclassified as observation and will not be reimbursed at observation rates.
CARC Code: A specific Claim Adjustment Reason Code (CARC) will identify these downgrades.
Appeals: If the concurrent discussion does not resolve the issue, providers may submit a formal appeal, following a process similar to DRG downgrade disputes.
Aetna will issue detailed guidance on October 15, 2025, outlining:
The review methodology (e.g., AI, nurse, or physician-driven)
Readmission handling
Specific reimbursement models/rates
Outstanding Questions & Clarification Needed:
Reapplication of MCG Criteria:
Will Aetna reapply MCG criteria during the course of the stay (e.g., for extended lengths or complications), or is the initial level-of-severity determination final regardless of hospital course?
CMS Regulatory Compliance:
According to 42 CFR § 422.566(d), CMS requires written notice of appeal rights to both beneficiaries and providers when services or payments are partially denied.
Definition of Medical Necessity:
CMS guidance explicitly states that denial terminology includes "medical necessity" and any substantively equivalent term (e.g., severity). Can Aetna bypass peer review and appeal processes simply by avoiding the term “medical necessity”?
Policy vs. Compliance Conflict:
In CMS Final Rule 4201-F, CMS clarified that payers may not avoid denial requirements by recasting medical necessity decisions as payment integrity issues. Does Aetna’s new policy conflict with this rule?
Contractual Reimbursement Terms:
Can Aetna legally apply this payment downgrade policy without amending DRG-based reimbursement terms in existing provider contracts?
Aetna’s upcoming Level of Severity Inpatient Payment Policy represents a significant operational and regulatory shift in how inpatient services for Medicare Advantage and SNP members are classified and reimbursed. While the policy aims to streamline approvals and reduce outright denials, it raises substantial compliance questions under CMS regulations regarding medical necessity determinations, appeal rights, and contractual payment terms. Hospitals should prepare for potential impacts on reimbursement integrity, utilization review workflows, and payer relations by reviewing their contract language, monitoring Aetna’s forthcoming implementation guidance, and seeking clarification from regulatory or legal experts to ensure alignment with federal requirements and patient protection standards.

Updates to CMS CoP Interpretive Guidelines: Discharge Planning
This early screening allows sufficient time to complete evaluations and develop discharge plans that truly support patient needs, goals, and preferences.
By Tiffany Ferguson, LMSW, CMAC, ACM
As alluded to on Monitor Mondays, Dr. Ronald Hirsch and I have been enjoying our fall lattes while combing through the Centers for Medicare & Medicaid Services (CMS) Conditions of Participation (CoP) Interpretive Guidelines.
The State Operations Manual (SOM), Appendix A – has new updates for hospitals in their QSO-25-24 release, thank goodness (because the last one was 2019-2020).
Although there are many updates in this version, I will be focusing on §482.43 Discharge Planning. I will preface this information with a healthcare reminder that “if you didn’t document it, you didn’t do it.” This will be important as I provide future updates, and as hospitals and healthcare system case management (CM) programs think about their processes.
One of the most notable changes is the strengthened emphasis on patient and caregiver participation in the discharge planning process. Hospitals must actively involve patients and their families in setting goals of care and treatment preferences. The discharge plan must not only reflect medical needs, but also incorporate patient values, cultural considerations, and post-discharge priorities. Surveyors will expect documentation that patients and caregivers were given meaningful opportunities to engage in decision-making and were informed of available post-acute options.
CMS reiterates that hospitals are responsible for early identification of patients who require discharge planning services. The updated guidelines clarify that the discharge planning process is expected to begin early in the hospitalization. Hospitals are directed to identify, upon admission, those patients who are likely to suffer adverse health consequences if discharged without adequate planning. This early screening allows sufficient time to complete evaluations and develop discharge plans that truly support patient needs, goals, and preferences.
The hospital’s policies and procedures must document the criteria and screening process used to identify patients who are likely to need discharge planning. These criteria should be evidence-based and clearly outline which staff are responsible for carrying out the evaluations. Importantly, CMS has clarified the survey standard: no noncompliance citations will be issued if identification is completed at least 48 hours in advance of discharge, provided there is no evidence that the delay resulted in harm.
The interpretive guidance also provides an important example. If a delay in screening results in discharging a patient to a nursing facility simply because such placements can be arranged quickly, when the patient preferred to go home and could have been safely supported with community services, this would represent a failure of timely identification. Even for hospital stays shorter than 48 hours, patients must still be screened promptly to ensure that discharge planning is completed before discharge, if needed.
This explanation reiterates CMS’s expectation that hospitals move away from last-minute discharge planning and instead adopt a proactive, patient-centered approach that maximizes safe and appropriate transitions of care. Additionally, the CM programs must have a mechanism for patients who were screened out initially as not having discharge planning needs, to be reassessed should the patient’s clinical condition change. It was also confirmed that should the physician request a discharge planning evaluation for their patient, one should be completed even if the patient did not meet the screening criteria.
The guidelines also specify that discharge planning evaluations must be conducted by, or under the supervision of, qualified personnel such as registered nurses, social workers, or other staff designated by hospital policy. This clarification ensures consistency and accountability in who performs and oversees these assessments. State law ultimately governs the qualifications necessary to practice as a registered nurse or social worker, but hospitals must further define in policy what constitutes “appropriately qualified” for other personnel engaged in discharge planning.
Importantly, the guidelines remind us that discharge planning is not a clerical or administrative task, but a specialized clinical function that requires both technical and interpersonal competence. CMS expects that all individuals conducting or supervising discharge planning, whether nurses or social workers, should demonstrate comprehensive knowledge across several domains, such as clinical considerations, social and behavioral factors, insurance coverage, and community resources.
Overall, now would be a good time to review your discharge planning policies and procedures to not only make sure they support the interpretive guideline updates, but also that there is a mechanism within your CM programs to ensure consistency across patients and staff.
When “Nowhere To Go” Becomes A Compliance Problem
As discharge delays and struggles continue with social and custodial issues, hospitals must strike a balance between patient care, regulatory compliance, and financial stewardship.
By Tiffany Ferguson, LMSW, CMAC, ACM
It is a common scenario that hospitals are grappling with patients who are medically ready for discharge but have no safe place to transition to. With post-acute beds at capacity, family limitations, and gaps in social support, these patients often remain in the hospital for days or even weeks, creating both financial strain and compliance risk. Recently, a health information management (HIM) coding professional asked a critical question: When patients are “discharged” from inpatient status but physically remain in the hospital, how should that be documented and coded?
To understand inpatient admissions and appropriate conversions to outpatient or discharge regulations, the starting point is CMS. Once a patient is admitted as an inpatient, they must remain in that status until discharge. Under 42 CFR § 412.4, an inpatient stay ends only upon discharge to home, death, or transfer to another licensed facility (such as a skilled nursing facility or swing bed). An inpatient who never physically leaves the hospital cannot be “downgraded” to outpatient in a bed (OPIB). Attempting to do so is not just an accounting maneuver, it undermines patient appeal rights and disrupts the proper application of MS-DRG reimbursement for the inpatient stay.
If we look at adjacent guidelines for the inpatient discharge process, we can see that CMS has a notification process for patients that are converted from inpatient to outpatient through the Condition Code 44 (CC44) process, which is intended for patients erroneously placed in inpatient. Additionally, with the role out of the Medicare Change of Status Notice (MCSN) it is very clear that CMS would want patients, if medically appropriate, to retain their inpatient designation to obtain their SNF benefits. A prolonged inpatient hospitalization, with a conversion to Outpatient in a Bed (OPIB) would sidestep these notices but also raise further ethical questions and remove the patient of their benefits to retain their inpatient admission or appeal their discharge. This would also raise questions as to why the patient was not discharged to a post-acute facility and instead stayed in an acute care facility that is not licensed appropriately to provide prolonged rehabilitation or custodial care for these patients.
I have also received questions about if it is possible to discharge the patient and then create a new encounter for the patient in the OPIB classification if they are inpatient. The answer is no; this practice is particularly concerning. If a patient is reported to CMS as discharged home but is, in fact, still residing in the hospital which is not licensed as a long-term care or residential facility, the hospital risks a licensing violation. Beyond compliance, this exposes patients to inappropriate billing practices and undermines the integrity of the discharge process.
So how should hospitals manage this dilemma?
Keep patients in inpatient status until true discharge: If they remain in the facility, they remain inpatient, even if their continued stay is no longer medically necessary.
Document avoidable days: Use internal tracking to note when patients are awaiting placement due to social factors. This transparency supports case management performance reporting and helps quantify the cost of “social delays.”
Engage leadership on capacity solutions: The root issue, lack of safe post-acute options, requires systemic solutions, not just coding workarounds.
As discharge delays and struggles continue with social and custodial issues, hospitals must strike a balance between patient care, regulatory compliance, and financial stewardship. Treating “nowhere to go” patients as outpatient boarders or prematurely coding them as discharged is not the answer. Instead, adherence to CMS rules, coupled with clear documentation of avoidable days, ensures compliance while spotlighting the urgent need for expanded post-acute resources. Ultimately, while social admissions may feel like a local operational problem, they are a national signal of system strain.

CMS FY26 IPPS Final Rule: Readmissions Expands To MA
CMS confirmed that beginning in FY 2027, the Hospital Readmissions Reduction Program (HRRP) will expand to include Medicare Advantage (MA) patients, not just traditional Medicare (FFS) beneficiaries.
By Tiffany Ferguson, LMSW, CMAC, ACM
The CMS FY 2026 Inpatient Prospective Payment System (IPPS) Final Rule is here, and case management leaders, as well as quality teams, should take note. The rule brings both confirmation of significant policy shifts and signals of what is coming in likely future rulemaking.
CMS confirmed that beginning in FY 2027, the Hospital Readmissions Reduction Program (HRRP) will expand to include Medicare Advantage (MA) patients, not just traditional Medicare (FFS) beneficiaries. This means the baseline data collection period will be from July 2023 to July 2025. The finalized updates include:
Refinement of all six readmission measures to incorporate MA patient cohort data.
Reduction of the applicable period from three years to two.
Codification of the Extraordinary Circumstances Exception (ECE) policy, giving CMS discretion to grant modifications.
Removal of the COVID-19 exclusion from all six readmission measures.
Notably, CMS decided not to finalize the inclusion of MA payment data in aggregate readmission penalty calculations, at least for now. The comments related to the inclusion of MA plans significantly expressed provider opinions and tone related to MA plans lack of payment for readmissions as well as their narrow networks which impact beneficiary access to care. Although CMS recognized this in their replies, they are focused on quality outcomes and the reality is that half of Medicare beneficiaries are in an MA plan and thus the data should include all Medicare beneficiaries.
An interesting mention in the readmission discussion and section was the use of “leave of absence” billing practices (Medicare Claims Processing Manual, Chapter 3, Section 40.2.5). Hospitals may place a patient on leave of absence when a readmission is expected but the patient does not require inpatient-level care during the interim. Importantly, this generates only one bill and one DRG payment, not two separate admissions.
As CMS evaluates readmission differences between FFS and MA populations, expect further attention around this practice, particularly as MA data become integrated into HRRP. It was unclear in the review exactly the significance of why this guideline was raised in the readmission option, but important to note.
CMS is also exploring refinements to readmission measurements, including:
Breaking down readmissions into 7-day and 14-day cohorts (not just 30-day).
Analyzing ambulatory care utilization and its relationship to readmission risk.
Separating readmission patterns across MA and FFS populations.
The FY 2026 IPPS ruling demonstrates CMS’s widening focus on readmissions, with Medicare Advantage now confirmed as ‘in scope’. For case management and quality leaders, the charge is twofold: Operationally, prepare for MA populations to be included in HRRP penalties, and strategically reexamine how data, discharge planning, and post-acute coordination will be managed under a shortened two-year reporting cycle.

Philosophical Changes from SDoH to Well-Being Measures
The data captured through social risk screenings is not simply a regulatory checkbox; it remains essential for ensuring safe and effective care transitions.
By Tiffany Ferguson, LMSW, CMAC, ACM
For this fall fashion season, the social determinants of health (SDoH) are out, and nutrition and well-being are in! Yet the parameters are not yet defined.
Arguably the most notable change in the Inpatient Prospective Payment System (IPPS) Final Rule for the 2026 fiscal year (FY) was the Centers for Medicare & Medicaid Services’ (CMS’s) decision to remove health equity as a pay-for-performance domain. This means that beginning at the end of this year, hospitals will no longer be required to conduct or submit data from the standardized five SDoH screening questions covering housing stability, utilities, personal safety, transportation, and food insecurity.
While the removal of federal reporting requirements reduces administrative burden, it simultaneously creates a new ethical dilemma for case management. The data captured through social risk screenings is not simply a regulatory checkbox; it remains essential for ensuring safe and effective care transitions.
For example, identifying unsafe living conditions is not optional; it directly ties to mandated reporting obligations that protect patient safety. Likewise, awareness of barriers such as food insecurity, utility shutoffs, or lack of transportation directly influences discharge planning and elevates the risk of readmission when left unaddressed. Housing instability has been shown to correlate strongly with inappropriate hospitalizations and extended lengths of stay, often driving costs higher while compromising patient outcomes.
In this way, the absence of a federal reporting mandate does not lessen the clinical and ethical responsibility of case managers. Instead, it challenges organizations to determine how they will continue capturing, documenting, and acting on these risk factors. Based on CMS’s responses to public comments, the agency has clarified that hospitals may voluntarily retain these screenings, even though they are no longer tied to federal reporting requirements. Thus, hospitals can choose to reframe these questions and data as internal quality metrics.
By repositioning these screenings as tools to inform care coordination, discharge planning, and readmission prevention, hospitals can continue to capture critical data that directly impacts patient outcomes. Ultimately, this approach could position case management and quality leaders to leverage the screenings for what they were always intended to do: illuminate barriers to safe transitions of care and reduce avoidable hospital utilization.
The Final Rule also included extensive commentary on potential well-being and nutrition measures for hospital reporting. While CMS did not adopt new requirements, they solicited and summarized significant stakeholder feedback.
Many commenters argued that well-being and nutrition measures are better suited for primary care or outpatient settings, not acute inpatient care. There were comments related to concerns from rural and resource-limited hospital leaders worried that such measures would be impractical and hold hospitals accountable for factors outside their control.
Regarding nutrition, many supported wider adoption of the Malnutrition Care Score (MCS) eCQM, with some recommending it be made mandatory. Commenters also highlighted food insecurity, diet quality, and hospital-community partnerships (e.g., medically tailored meals, food pharmacies) as vital to discharge planning and long-term health. Suggestions also pushed for a rephrasing of the conversation to outcome-based measures reflecting improvements in health and quality of life, similar to an alignment with SDoH screening. It’s kind of like a rebrand of SDoH as well-being!
CMS did not issue new mandates in FY 2026, but noted that this feedback will inform future measure development for the Hospital Inpatient Quality Reporting (IQR) Program.

CMS Releases 2025 Fast Facts On Hospice Program Integrity
In the review for FY 2024, CMS identified concerning trends, including improper billing and hospices not being fully operational at their registered addresses.
By Tiffany Ferguson, LMSW, CMAC, ACM
The Centers for Medicare & Medicaid Services (CMS) recently published a concise “Hospice Fast Facts,” which provides key insights into hospice utilization in the 2024 fiscal year (FY), Medicare payment volumes, and program integrity initiatives.
In the one-sheet paper, we see that Medicare hospice spending exceeded $27 billion in FY 2024, and that roughly 1.8 million Medicare beneficiaries received hospice care during that period. Although the document emphasized that hospice is an essential benefit within the Medicare program, many of the bullet items discussed the concern regarding potential overutilization of hospice services.
For reference, hospice providers are reimbursed on a per‑diem basis, with rates varying according to the type of care delivered, ranging from routine home care to continuous home care, general inpatient care, or inpatient respite care.
The document appears to align with CMS’s expanding program integrity efforts to curb fraud, waste, and abuse among Medicare‑enrolled providers – and in this case, hospice providers. The Center for Program Integrity (CPI) is leading these initiatives, utilizing enforcement actions, provider education, and targeted audits to ensure that program funds are used appropriately.
In the review for FY 2024, CMS identified concerning trends, including improper billing and hospices not being fully operational at their registered addresses. In response to this, they have initiated site visits, claim reviews, and administrative actions for identified hospice agencies that are being flagged with potential concerns for program integrity.
CMS notes that hospice utilization and expenditures have steadily increased in recent years. This growing financial footprint invites heightened oversight, especially as CMS balances access to end‑of‑life care with safeguarding taxpayer dollars. For hospice administrators, clinicians, and compliance officers, the fact sheet serves as a critical reminder of the importance of operational transparency, accurate provider enrollment, and address validation.
It is also important to see how there will likely be ongoing scrutiny of hospice agencies from CPI via audits, reviews, and potential enforcement.
Now would be an important time to proactively review the patient referral and acceptance process, documentation, and billing standards.
While the fact sheet does not delve into future payment update proposals, it complements broader CMS policy initiatives such as upcoming proposed rules for the FY 2026 hospice wage index, payment update percentages, and quality reporting requirements. These forthcoming rules will determine next year’s payment rates, hospice cap limits, and revisions to regulations around physician certification and quality reporting requirements.

Case Management Corner: A Nurse Case Manager or a Social Work Case Manager?
While case management was once primarily the domain of nurses, who perceived the job as a step up from the bedside, that changed during the COVID-19 pandemic.
By Kelly Bilodeau
Nurse case managers and social workers were once a natural pairing, working in tandem to support the patient.
“The idea was that nurses would handle medically complex issues while social workers would focus on social needs,” said Tiffany Ferguson, LMSW, CMAC, ACM, CEO of Phoenix Medical Management Inc.
However, due to changing paradigms and a more challenging patient population, case managers and social workers today often find themselves stepping on each other’s toes, and it’s becoming increasingly clear that it’s time to rethink traditional roles, she said.
A Changing Role
Case management is undergoing a transformation, thanks to patient and care-related changes. “Length of stay is shorter. We’re more efficient,” Ferguson said. “Patients are simultaneously medically and socially complex.” A case manager needs to be able to handle both aspects.
While case management was once primarily the domain of nurses, who perceived the job as a step up from the bedside, that changed during the COVID-19 pandemic. Hospitals were forced to make nursing jobs more appealing to retain and attract staff members during the crisis.
“Now the incentives for a floor nurse are way better than they are for a nurse case manager,” says Ferguson. Not surprisingly, fewer nurses are making the shift. Instead, when many floor nurses decide to leave the bedside they are selecting remote positions or to pursue advanced training to become nurse practitioners, she said.
At the same time, case management has become increasingly appealing to social workers. “There’s an ample pool of social workers who are coming into the marketplace and want to work in healthcare,” Ferguson said. They’re stepping into roles at hospitals that are either a split nurse/social worker model. “Or they could be doing the same exact job as a nurse case manager,” Ferguson said.
Rethinking Hiring
To solve these issues, directors need to stop thinking about whether it’s best to hire a nurse or a social worker and instead start hiring the individual with the most potential as a case manager. This is someone with solid social skills who works well at the patient’s bedside and can communicate effectively with floor nurses, physical therapy staff, and physicians. “They have to be a go-getter, really autonomous at filling their day and getting everything accomplished with patients. They have to have good boundaries, and be skilled with technology,” Ferguson said.
From there, training can fill the gaps.
For a social worker, an onboarding program might focus on how to handle the medical complexities of the role, anticipating care pathways, medication protocols, and navigating prior authorization requirements.
Conversely, a nurse may need more education on social factors. However, as nursing becomes increasingly specialized, these candidates may perform some, but not all, aspects of care. They may also need additional training on how medical conditions and care plans translate to proactive transitional needs for the patient. For example, at many facilities, discharge and admission are handled by separate team members, so a bedside nurse may no longer be as adept at performing a history and physical or in anticipating the patient’s post-acute needs.
“It's not like it used to be where one nurse did all of it,” Ferguson said.
Onboarding and orientation should be tailored to the individual. “You can't assume based on the person's professional license that they're going to come in skilled enough and know how to do the job,” Ferguson said. The job has grown so challenging that even an adept case manager requires continual ongoing training to stay up to date, she said.
Overall, hiring decisions should no longer be about choosing between a nurse and a social worker. It’s about identifying adaptable, skilled professionals and giving them the tools they need to succeed, Ferguson said.
Case Management Corner is your go-to source for insightful discussions on relevant topics in case management. Through an engaging interview-style format, our team members share their expertise, experiences, and best practices to keep you informed and empowered. Whether you're looking for industry updates, practical strategies, or real-world perspectives, we bring you valuable conversations designed to enhance your knowledge and support your professional growth. Stay tuned for expert insights straight from the field! Kelly Bilodeau has been a longtime writer for HCPro’s Case Management Monthly.

Ensuring Compliance with Condition Code W2 and 44 Processes
This clearly states that hospitals may not default to CC44 or CCW2 to address lack of utilization review (UR) coverage, physician advisor coverage, or medical staff education about patient status assignment. Unfortunately, this continues to be a strategy for many hospitals challenged with staffing limitations.
By Juliet Ugarte Hopkins, MD, ACPA-C
Condition Code W2 (CCW2), referred to by some as a “Medicare self-denial” or “Medicare Part B rebilling,” has been around for over a decade, since it was initially referred to in Chapter 6 of the Medicare Benefit Policy Manual. Dr. Alvin Gore, member of the Emeritus Board of the American College of Physician Advisors, wrote for RACmonitor.com back in May 2019, comparing CCW2 to Condition Code 44 (CC44). He recommended hospitals attempt to utilize the latter process over the former, opining that the CC44 process was more efficient, from a billing and reimbursement standpoint, and more transparent, from a patient status standpoint.
I agree with Dr. Gore, and also refer to the Centers for Medicare & Medicaid Services (CMS) direction in the Federal Register from August 2013, which includes the following:
“Use of Condition Code 44 or Part B inpatient billing pursuant to hospital self-audit is not intended to serve as a substitute for adequate staffing of utilization management personnel or for continued education of physicians and hospital staff about each hospital’s existing policies and admission protocols. As education and staffing efforts continue to progress, inappropriate admission decisions, and the need for hospitals to correct inappropriate admissions or report Condition Code 44, should become increasingly rare.”
This clearly states that hospitals may not default to CC44 or CCW2 to address lack of utilization review (UR) coverage, physician advisor coverage, or medical staff education about patient status assignment. Unfortunately, this continues to be a strategy for many hospitals challenged with staffing limitations.
Similarly, hospitals must ensure that they are compliantly following all of the steps in the CC44 and W2 processes. In 2021, I wrote in-depth about CC44, deconstructing the concepts between the code itself and the mandated Medicare process. While the CCW2 process applies to Medicare cases only, it’s imperative to understand that the details must be followed, no matter how complex and daunting they feel to carry out. Indeed, as Dr. Gore illustrated in 2019, the CCW2 process is complicated and time-intensive. However, it’s also mandated by CMS – and is not optional.
A common practice for retrospective “Medicare short stay” reviews involves Medicare patients discharged from the hospital in inpatient status following a hospitalization lasting fewer than two midnights. I believe that best practice extends this sampling to patients hospitalized for fewer than three midnights, capturing potential cases wherein an overzealous clinician or utilization manager changed the patient’s status to Inpatient solely based on the passage of a second midnight, without considering the medical necessity.
CMS notes that there are specific caveats to the Two-Midnight Rule, including death, transfer to a higher level of care, and others, wherein inpatient billing is still appropriate, even if the hospitalization did not involve at least two midnights. Following review by an experienced utilization nurse, these cases should pass along to billing for completion as-is. Tricky cases, where it’s not clear if the patient who left against medical advice (AMA) early in the morning on hospital day two actually had a condition supporting a two-midnight anticipation on hospital day one, or all of the cases for which the “patient improved more quickly than anticipated” is referenced in the documentation, should be referred to a physician advisor for additional review.
If the physician advisor does not feel that the documentation supports a two-midnight anticipation, which would support Medicare re-billing under Part B, they must reach out to the physician who entered the inpatient order. Notification need not be lengthy, but should include the following points:
Retrospective review of the case does not find a two-midnight anticipation was warranted and (briefly) why;
The hospital plans on billing the case as outpatient to Medicare Part B instead of inpatient to Medicare Part A, but this does not affect or apply to provider billing;
The physician has an opportunity to disagree with the decision and must respond to request further discussion with the physician advisor by a specific deadline; and
If the deadline passes and there is no response from the physician, Part B re-billing will proceed.
In the event the physician disagrees, there must be a discussion between her/him and the physician advisor. If the physician provides additional information that persuades the physician advisor that inpatient billing criteria was met, the physician advisor should pass the case along for Medicare Part A billing and advise the physician to include the missing clinical information in their H&P, progress note, or discharge summary, as appropriate. If the physician and physician advisor continue to disagree, a second physician on the hospital’s utilization management committee (UMC) should be required to review the case and weigh in. If this second UR physician agrees with the clinician that inpatient status was supported, the claim goes forward with Medicare Part A billing. If the second UR physician agrees with the physician advisor, the claim is re-billed to Medicare Part B.
Finally, patients associated with claims re-billed to Medicare Part B must be notified by the hospital. This can be automated within the electronic health record, utilizing a templated letter format, but should include information about where and how the patient can contact the hospital to discuss the situation, if they wish.
How is your hospital reviewing and managing CCW2s? Is your physician advisor or other physician member of the UMC involved? Are attending physicians receiving notification and allowed a chance to respond? Are patients notified of the change in their claim? If you’re not sure, I encourage you to investigate and confirm that the process is being followed compliantly.

The CMS WISeR Model: A Targeted Approach To Expand Prior Auths
WISeR is the first push to pair broad-scale, claims-based utilization analytics with Medicare Administrative Contractor (MAC)-directed pre-payment medical necessity review for professional and outpatient services.
By Tiffany Ferguson, LMSW, CMAC, ACM
The Centers for Medicare & Medicaid Services (CMS) has announced the establishment of the Wasteful and Inappropriate Services Elimination and Reduction (WISeR) Model, a six-year initiative launching Jan. 1, 2026.
This so-described voluntary model (although in reading the guidelines, it becomes clear it is very much mandated for the six states) introduces a structured, technology-enabled approach to prior authorization and pre-payment review for selected Medicare Part B services deemed to be of low clinical value, overused, or associated with fraud, waste, and abuse.
The WISeR Model represents a significant evolution in the CMS oversight strategy. Historically, the use of prior authorization by Medicare has been limited to targeted service categories such as durable medical equipment (DME), non-emergency transportation, or certain outpatient procedures. WISeR is the first push to pair broad-scale, claims-based utilization analytics with Medicare Administrative Contractor (MAC)-directed pre-payment medical necessity review for professional and outpatient services.
As noted, WISeR will be implemented across six states: New Jersey, Ohio, Oklahoma, Texas, Arizona, and Washington. These states were selected based on Medicare volume, geographic diversity, and alignment within four existing MAC jurisdictions:
JL (New Jersey);
J15 (Ohio);
JH (Oklahoma, Texas); and
JF (Arizona, Washington).
Each participating state will serve as a testing ground for evaluating changes in service utilization, program integrity, and cost savings.
Providers in the six participating states will be required to either submit prior authorization requests for these services or accept a pre-payment review upon claim submission. Instead of the MACs, from the ruling, CMS will be using designated contractors, under MAC oversight, that will determine whether claims meet established medical necessity criteria. The ruling also mentioned the provision of this group to utilize artificial intelligence (AI)-enabled tools.
The specific procedures and devices that CMS has identified include the following:
Electrical Nerve Stimulators (NCD 160.7);
Sacral Nerve Stimulation for Urinary Incontinence (NCD 230.18);
Phrenic Nerve Stimulator (NCD 160.19);
Deep Brain Stimulation for Essential Tremor and Parkinson’s Disease (NCD 160.24);
Vagus Nerve Stimulation (NCD 160.18);
Induced Lesions of Nerve Tracts (NCD 160.1);
Epidural Steroid Injections for Pain Management excluding facet joint injections (L39015, L33906, L39036, L39240, L39242, L36920, L38994, L39054);
Percutaneous Vertebral Augmentation (PVA) for Vertebral Compression Fracture (VCF) (L33569, L34106, L34228, L38201, L34976, L35130, L38737, L38213);
Cervical Fusion (L39741, L39799, L39770, L39758, L39762, L39793, L39773, L39788);
Arthroscopic Lavage and Arthroscopic Debridement for the Osteoarthritic Knee (NCD 150.9);
Hypoglossal Nerve Stimulation for Obstructive Sleep Apnea (L38276, L38307, L38398, L38387, L38310, L38312, L38385, L38528);
Incontinence Control Devices (NCD 230.10);
Diagnosis and Treatment of Impotence (NCD 230.4);
Percutaneous Image-Guided Lumbar Decompression for Spinal Stenosis (NCD 150.13);
Skin and Tissue Substitutes (LCDs below) – only applicable to MAC jurisdictions and states that have an active LCD in place;
Application of Bioengineered Skin Substitutes to Lower Extremity Chronic Non-Healing Wounds (L35041); and
Wound Application of Cellular and/or Tissue Based Products (CTPs), Lower Extremities (L36690).
An interesting consideration in the ruling, mentioned as an exploration, is the CMS provider safeguard known as “provisional affirmation.” If a claim is not affirmed, providers would receive a detailed rationale and may resubmit or appeal the determination.
Additionally, organizations demonstrating an affirmation rate of more than 90 percent over time may qualify for a gold-carding exemption, temporarily removing them from the prior authorization requirement, similar to commercial plans.
Financially, CMS will compensate the third-party reviewers not on volume, but based on a share of the Medicare expenditures they help avert, ensuring alignment with the CMS goals of reducing low-value care and reducing waste.
While inpatient services are not directly subject to the model, the ripple effects on outpatient surgery, interventional procedures, and medical device utilization will require cross-functional coordination. Surgical locations will want to have a clear understanding of the required medical guidelines for procedural authorization and approval. Clear, evidence-based documentation will be critical for both prior authorization requests and appeals.
WISeR reflects the CMS continued movement toward proactive utilization management, with an invested approach toward leveraging technology and a commercial payer approach. While the model is currently limited to six states and select services, its structure suggests a potential framework for broader application.

CMS Transitions Inpatient Hospital Short-Stay Reviews to the MACs
This realignment allows QIOs to focus on broader quality improvement initiatives, while MACs, already responsible for various audit and compliance efforts through the existing Targeted Probe-and-Educate (TPE) program, will bring greater oversight to short-stay reviews.
By Tiffany Ferguson, LMSW, CMAC, ACM
I’d like to begin with a thank-you to Dr. Stephanie Van Zandt, Medical Director of Physician Advisor Services at BayCare, for sharing this news.
The Centers for Medicare & Medicaid Services (CMS) is shifting the responsibility for inpatient hospital short-stay reviews from the Beneficiary and Family Centered Care Quality Improvement Organizations (BFCC-QIOs) to the Medicare Administrative Contractors (MACs), effective Sept. 1. According to the Inpatient Hospital Reviews FAQs | CMS, the justification for this change is to allow the BFCC-QIOs (Acentra Health and Livanta) to focus their efforts on quality improvement and expedited appeals.
With the additional time afforded to the BFCC-QIOs, they will be shifting their focus to other quality-related functions, such as higher-weighted DRG reviews, hospital discharge appeals, and quality-of-care concerns. This realignment allows QIOs to focus on broader quality improvement initiatives, while MACs, already responsible for various audit and compliance efforts through the existing Targeted Probe-and-Educate (TPE) program, will bring greater oversight to short-stay reviews.
The inclusion for prepayment reviews on hospital short stays will now be prioritized for review under the MAC-led Targeted Probe and Educate (TPE) program. According to the FAQs from CMS, a hospital short stay is defined as a length of stay that is fewer than two midnights after inpatient admission. While such admissions may be clinically appropriate, CMS has identified them as having a higher risk category for improper payments. These reviews will be performed by registered nurses (RNs) with available access to the MAC’s medical director(s).
These reviews will evaluate patient status documentation to ensure that each patient’s condition supports the need for inpatient hospital services, in accordance with 42 C.F.R. § 412.3(d) and not proprietary commercial screening tools like InterQual or MCG.
MACs will apply the existing TPE program, which uses data analytics to identify providers with outlier billing patterns. MACs will conduct these reviews on a prepayment basis, giving providers the ability to rebill Part B when Part A payment is denied, or pursue the further appeals should the provider disagree, in accordance with the Medicare appeals process. According to the details, this prepayment review will be completed with a sample of 20-40 claims per provider, as a round of review. Providers may have a total of up to three rounds before they are referred to CMS for additional administrative action.
CMS and the MACs have outlined an implementation plan that includes educational outreach, updated guidance in the Program Integrity Manual, and MLN communications. This transition will not change CMS’s patient status policies, nor diminish the importance of a physician’s clinical judgment. However, hospitals must now ensure that documentation clearly supports the need for inpatient care under the two-midnight rule. With MACs leading these reviews, providers can expect more targeted oversight, demonstrating CMS’s commitment to reduce waste and abuse.

New Requirements in CMS’ Conditions of Participation Regulations
While the transfer of patients between hospital units or facilities has long been a routine operational function, CMS is now moving to standardize and elevate the practice as a core compliance obligation, focused on improving patient safety, care transitions, and timely access to appropriate levels of care.
By Tiffany Ferguson, LMSW, CMAC, ACM
Effective July 1, a subtle but significant expansion for the Centers for Medicare & Medicaid Services (CMS) added new requirements to 42 CFR § 482.43 regarding transfer protocols. Originally mentioned back in November 2024 as part of the CY 2025 Outpatient Prospective Payment System (OPPS) Final Rule, CMS announced the finalization of new requirements in conjunction with the maternal healthcare news briefs.
However, likely during the political change of offices, an interesting proactive statement was added to the Conditions of Participation (CoP) regulations that require acute-care hospitals to develop and implement written transfer protocols.
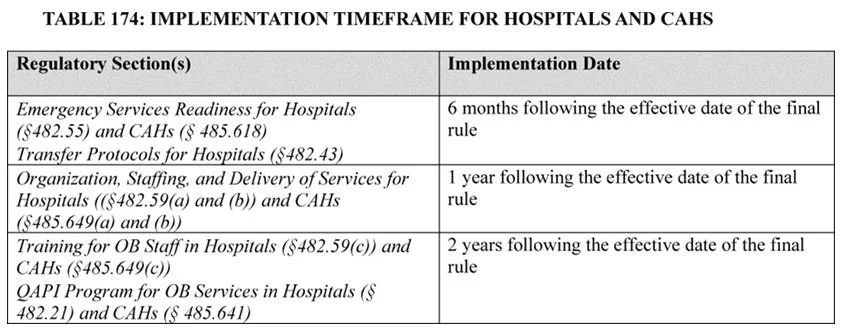
The finalized regulation, outlined in § 482.43(c), mandates that all acute-care hospitals have written policies and procedures governing intra-hospital and inter-hospital transfers. These include the following:
Transfers from the emergency department to inpatient admission;
Transfers between units within the same hospital; and
Transfers between different hospitals for higher levels of care or specialized services.
While the transfer of patients between hospital units or facilities has long been a routine operational function, CMS is now moving to standardize and elevate the practice as a core compliance obligation, focused on improving patient safety, care transitions, and timely access to appropriate levels of care. This rule codifies what many hospitals already do, transferring patients from the ED to hospitalized patient units, between units, and to other facilities. But now, these processes must be formally documented in written policy, implemented organization-wide, and supported with annual training for designated staff.
Hospitals are also required to conduct annual training for relevant staff on these transfer protocols. Notably, CMS leaves flexibility for hospitals to determine which staff are included, allowing adaptation based on organizational structure and resources.
However, given the unique ties of this additional standard with obstetrics, consideration should be given to hospital admissions and transfers in and out of the mother-baby unit. For hospitals to ensure appropriate compliance, it makes sense to audit and formalize existing transfer policies.
Consider review of the existing annual training provided to applicable clinical staff to meet the requirements for providing information regarding transfer protocols.
In reviewing the original guidance and comments in the CY 2025 OPPS ruling as to what led to this change, CMS cited the need to reduce delays, ensure continuity, and protect patients in particularly vulnerable populations, such as pregnant and postpartum individuals. Federal Register :: Medicare and Medicaid Programs: Hospital Outpatient Prospective Payment and Ambulatory Surgical Center Payment Systems; Quality Reporting Programs, Including the Hospital Inpatient Quality Reporting Program; Health and Safety Standards for Obstetrical Services in Hospitals and Critical Access Hospitals; Prior Authorization; Requests for Information; Medicaid and CHIP Continuous Eligibility; Medicaid Clinic Services Four Walls Exceptions; Individuals Currently or Formerly in Custody of Penal Authorities; Revision to Medicare Special Enrollment Period for Formerly Incarcerated Individuals; and All-Inclusive Rate Add-On Payment for High-Cost Drugs Provided by Indian Health Service and Tribal Facilities

Case Management Corner: Why Are Case Managers Using The Same, Tired Framework?
The Adaptive Model follows patients into the emergency department, pre-surgical and hospitalized outpatient units, and even into their homes using telehealth.
By Kelly Bilodeau
Today’s case managers have digital tools, value-based goals, and post-pandemic challenges. So why are they still relying on a 1990s playbook?
For decades, hospitals have used the Triad Model: a case manager, social worker, and utilization review specialist committed to getting the patient out of the hospital as quickly and efficiently as possible, according to Marie Stinebuck, MBA, MSN, ACM, COO at Phoenix Medical Management Inc. However, as patient complexity rises, staff numbers shrink, and goalposts shift, this three-legged structure is buckling under modern demands, said Tiffany Ferguson, LMSW, CMAC, ACM, CEO of Phoenix Medical Management.
It’s time for a new framework—the Adaptive Model, which Ferguson recently outlined in an article for CMSA Today.
Navigating post-COVID challenges
Many hospital officials recognize that the Triad Model is a problem, Ferguson said in a recent Finally Friday webinar.
“People are coming to us saying, ‘We need to look at this model. I don't think we have the right staffing mix,’” she said.
Job responsibilities feel muddled. Case managers and social workers often have overlapping responsibilities, which creates redundancies and confusion for patients. The Utilization Review (UR) role evolved significantly during COVID, as many positions transitioned to remote work. This shift altered the dynamics and collaboration within the inpatient care team. These factors put a drag on efficiency in a department that is already often understaffed and overburdened following a surge in pandemic-driven retirements.
At the core of these issues is an outdated system, way overdue for an update.
“Until readmissions became a key focus around 2012, case management remained primarily centered on discharge planning," Stinebuck said.
Since that time, hospitals have adopted integrated technology, including automated workflows and AI-driven case management software, and added post-acute partners. However, the foundational model hasn’t caught up.
Moving to a new approach
Where the Triad Model falls short in promoting proactive pre-hospitalization planning or addressing the social needs of patients, the Adaptive Model excels. It helps to eliminate redundancies between case management and social work.
“This new Adaptive Model looks at those roles. How do we complement each other without overlapping and work in the best interest of that patient?” Stinebuck said.
It also expands the tent, incorporating new team members, such as the physician advisor, a position formalized after the Triad Model’s inception, and non-licensed professionals. These non-licensed staff members reduce the burden on case managers by handling routine administrative tasks like scheduling outpatient appointments, arranging transportation, and delivering regulatory notices. This frees case managers to focus on more critical aspects of patient care and new goals, such as readmission prevention, addressing social determinants of health, and meeting value-based care targets.
The Adaptive Model also recognizes the time-saving value of integrated technology and expands interventions beyond inpatient units. Care has changed. The Adaptive Model follows patients into the emergency department, pre-surgical and hospitalized outpatient units, and even into their homes using telehealth.
Making the shift
Now, the goal should be to make changes that help case management meet patient needs in a world where efficiency is more crucial than ever. Case management no longer starts and ends in the hospital. Planning begins before admission, extends after discharge, and goes beyond simply pushing people through the system. The Adaptive Model is patient-centered and offers case managers the tools and the bandwidth to meet their needs at a time when demands often outstrip resources.
The old model is costing hospitals “time, money, and sanity,” said Ernie de los Santos, host of the Finally Friday webinar. It’s time to transition. The shift to the Adaptive Model isn’t just an evolution, “it’s a survival strategy,” he said.
Case Management Corner is your go-to source for insightful discussions on relevant topics in case management. Through an engaging interview-style format, our team members share their expertise, experiences, and best practices to keep you informed and empowered. Whether you're looking for industry updates, practical strategies, or real-world perspectives, we bring you valuable conversations designed to enhance your knowledge and support your professional growth. Stay tuned for expert insights straight from the field! Kelly Bilodeau has been a longtime writer for HCPro’s Case Management Monthly.

CMS Crackdown on Medicaid Coverage for Undocumented Patients Raises Red Flags
Patients who are medically ready for discharge but unable to access follow-up care due to immigration status or lack of funding may face extended hospital stays.
By Tiffany Ferguson, LMSW, CMAC, ACM
In a significant policy shift with wide-ranging implications for healthcare operations, the Centers for Medicare & Medicaid Services (CMS) announced that it will ramp up enforcement actions against states that use federal Medicaid dollars to provide healthcare to undocumented immigrants. This initiative, tied to a broader executive order focused on ending “taxpayer subsidization of open borders,” signals a more aggressive posture from the federal government and threatens to reshape how hospitals care for vulnerable patient populations.
While federal law has long restricted Medicaid funding to cover only emergency medical services for noncitizens without legal immigration status, CMS contends that states have stretched those definitions – often in the interest of delivering humane, cost-effective care. But under this new directive, such flexibility may soon come at a cost.
“Medicaid is not, and cannot be, a backdoor pathway to subsidize open borders,” said CMS Administrator Dr. Mehmet Oz in a press release. “We are putting states on notice – CMS will not allow federal dollars to be diverted to cover those who are not lawfully eligible.”
What’s Changing: Increased Oversight and Financial Consequences
As part of its enhanced oversight, CMS will begin focused audits of state Medicaid spending (CMS-64 reports), conduct in-depth reviews of financial systems, and assess eligibility rules to identify improper payments. The goal is to recoup federal matching funds from states that are out of compliance. CMS is also calling on states to urgently update internal controls, eligibility systems, and cost allocation policies.
These enforcement actions are expected to hit hardest in states that have, either through interpretation or legislative action, expanded Medicaid-funded emergency services to include treatments that CMS now deems outside the bounds of federal law.
States Like Arizona in the Crosshairs
Arizona offers one such example. The state has extended emergency Medicaid to include outpatient dialysis for undocumented individuals with end-stage renal disease (ESRD). Without access to routine dialysis, these patients would be forced into emergency-only care – a practice shown to increase hospital admissions, mortality rates, and healthcare costs.
The rationale behind Arizona’s policy, shared by several other states, including California, Illinois, and New York, is both humanitarian and practical: it reduces the frequency of emergency department visits, improves patient outcomes, and saves money by preventing crisis-driven care. However, under CMS’s new guidance, these expenditures may be deemed improper and subject to federal clawbacks.
This presents a critical challenge for Medicaid administrators and hospital systems: comply with stricter federal mandates or continue providing life-sustaining care with the risk of losing reimbursement.
Hospitals and Case Managers Face a Discharge Dilemma
Hospitals, especially those serving immigrant-heavy communities or functioning as safety-net providers, are already feeling the ripple effects. Case managers, who coordinate discharge plans and post-acute care transitions, routinely depend on emergency Medicaid to fund services such as skilled nursing facility transfers, home health services, and dialysis for undocumented patients. If CMS disallows these services, discharge planning becomes significantly more complex.
Patients who are medically ready for discharge but unable to access follow-up care due to immigration status or lack of funding may face extended hospital stays. This not only inflates length-of-stay metrics and strains inpatient capacity, but also creates financial burdens through uncompensated care. Alternatively, hospitals may be forced to discharge patients without adequate support, raising ethical concerns and increasing the risk of readmissions or poor health outcomes.
As CMS enforces tighter boundaries, case managers must rethink their workflows, collaborate more intensively with legal teams and charity care coordinators, and explore non-traditional partnerships with nonprofit organizations and faith-based groups to ensure that patient needs are met.
Medical Repatriation: A Legal and Ethical Minefield
When no viable discharge option exists in the U.S., hospitals may turn to medical repatriation: the practice of returning a patient to their country of origin for continued care. While not new, this approach is controversial, and raises significant ethical, legal, and reputational risks.
Increased federal scrutiny could unintentionally make repatriation more common. Patients who require long-term ventilator care, dialysis, or rehabilitation but have no insurance, public coverage, or family support may be identified as candidates for international transfer. However, this process is not straightforward. It requires coordination with foreign consulates, identification of a receiving facility abroad, and, ideally, the patient’s informed consent.
Legal advocates have long criticized repatriation as coercive when driven by hospital financial pressures rather than patient choice. Many patients may have lived in the U.S. for decades, have no access to care in their country of origin, or fear returning due to political instability or lack of support systems.
Still, without coverage options, hospitals may find themselves forced to explore every alternative – even those that would have once seemed untenable.
Fiscal and Ethical Tensions
Hospitals are caught between compliance mandates and their duty of care. In states like Texas, where a 2024 report estimated over $121 million was spent in a single month treating undocumented patients – and $25 million tied to Medicaid or CHIP – the potential financial impact of recoupments is enormous. For hospitals, that could mean reducing charity programs, downsizing staff, or shifting more uncompensated care onto the general operating budget.
At the same time, the directive undermines public health strategies that depend on early intervention and consistent care for chronic conditions. From a case management perspective, limiting emergency Medicaid to the strictest possible definition may seem fiscally prudent in the short term, but it ultimately drives up system-wide costs through avoidable hospitalizations, preventable complications, and legal challenges.
Looking Ahead: Preparing for a New Era of Compliance
Hospitals and health systems must begin preparing now. That includes:
Reassessing current discharge planning protocols for undocumented patients;
Training staff on the narrower definitions of Medicaid-covered emergency services;
Evaluating the legal, ethical, and operational implications of repatriation; and
Strengthening partnerships with community organizations, charity clinics, and legal aid groups.
The CMS crackdown is not just a bureaucratic shift; it’s a redefinition of how care is delivered to one of the most vulnerable populations in the U.S.
For hospitals and case managers, navigating this evolving terrain will require adaptability, ethical clarity, and a renewed focus on advocacy-driven care planning.

Embrace Your Physician Advisors’ Potential
Juggling patient care and potentially one or two other administrative roles can prevent these physicians from developing the level of expertise and familiarity they need to effectively function as a physician advisor.
By Juliet Ugarte Hopkins, MD, ACPA-C
The role of physician advisors has evolved into an absolute necessity in hospitals of all sizes around the country. As the healthcare landscape rapidly evolves, physician advisors have proven to serve as critical players, bridging the gap between confusion and clarity within clinical and administrative functions.
The role started as a loosely defined physician champion for case and utilization management teams. Only one or two individuals on a hospital’s medical staff generally gravitated to this position, usually as they were winding down in their career and looking to work fewer clinical hours. But, with the arrival of the Medicare Inpatient-Only list in 2000, nationwide Recovery Audit Contractor (RAC) audits in 2009, and creation of the Medicare Two-Midnight Rule in 2013, a new spotlight on hospital compliance, with mandates related to Centers for Medicare & Medicaid Services (CMS) rules and regulations, came into being.
As more and more physicians became well-versed in hospital service utilization, payment structures, and potential penalties related to compliance and quality metrics, these individuals moved beyond serving as mere support for nurse case and utilization managers. They were tasked with translating CMS requirements and payor guidelines about medical necessity and documentation to their colleagues in a way they could understand and put into practice. While undoubtedly frustrating, it increasingly became clear that a message about “the business of medicine” delivered to medical staff by a physician was received much more readily than the same message conveyed by a non-physician.
In 2014, a number of these individuals – now with the common title of Physician Advisor – came together to form the American College of Physician Advisors (ACPA). This nonprofit, physician-led organization is now home to over 1,200 members, and serves as a testament to the evolution of the field. Physician advisors are now experts for adult and pediatric populations not only in case and utilization management, but also clinical documentation integrity, population health, quality initiatives and strategies, and much more. This role is an essential part of Condition Code 44 and W2 processes, which cannot be overlooked, from a compliance perspective. When considering hospital viability, in light of aggressive payor tactics involving medical necessity denials and DRG downgrades, physician advisors are particularly effective working with utilization management (UM) and clinical documentation integrity (CDI) leadership, in collaboration with medical staff.
While the role of physician advisor began as perhaps only one individual in a hospital who took on the rapidly growing needs of case and utilization management departments, a new staffing model has recently grown in popularity. More and more, hospitals are attempting to fulfill their needs by employing multiple physicians in fractions of full-time equivalents (FTEs) devoted to the physician advisor role. Instead of one physician working full-time, five rotate over the course of the month, assigned only 0.2 FTE for the efforts. Often, this leads to significant reduction of the focus and level of expertise provided by these physician advisors. Juggling patient care and potentially one or two other administrative roles can prevent these physicians from developing the level of expertise and familiarity they need to effectively function as a physician advisor. Especially in situations where they are never working with 100-percent focus on their physician advisor role – for example, when the vice president of medical affairs or medical director of a large hospitalist group is also serving as the physician advisor – it is almost impossible to address status escalations in a timely fashion or find time for creation and provision of routine education for medical staff and UM teams.
If a hospital feels they can’t secure full-time physician advisors because there are individuals within the organization who are genuinely interested in the role, but aren’t ready to give up their clinical work, they should establish a full-time lead or chief physician advisor. This role will serve as the glue and ringmaster for the hospital’s physician advisory efforts, ensuing there is a consistent go-to person all staff is familiar with and relies on, no matter what the situation, day of the week, or time of day. Free from secondary review escalations, this individual can focus on studying data related to metrics such as medical necessity denials by payor according to primary diagnosis, readmissions, and utilization of Condition Code 44 and W2. The lead would also be responsible for ensuring the continuous education and proficiency of the other physician advisors on the team, including providing onboarding and mentoring support when new members are added. As physician advisors become exponentially more common and valuable within hospitals and health systems, it’s important to understand how their impact can be inadvertently diluted through FTE spread. Consider combating against this by establishing a full-time lead physician advisor, or mandating that each physician serving in the role works at least 0.5 FTE, to ensure persistent mastery of and focus on the subject matter.

Case Management Corner: Trauma-informed Approach Improves Care For Patients
In the past, providers often dismissed trauma-induced outbursts as bad behavior or a character flaw.
By Kelly Bilodeau
A hospital visit can be a stressful experience for anyone, but it may be particularly overwhelming for the more than 50% of Americans with a history of trauma. For those who have endured physical or emotional abuse, medical encounters can trigger panic, complicating treatment and sometimes leading to emotionally volatile encounters that can put medical staff members at risk.
“As a trauma therapist and clinical social worker in the emergency department, I often witness how standard medical practices can inadvertently retraumatize patients. Trauma-informed care transforms these encounters, allowing us to offer not just treatment, but healing,” said Kalie Wolfinger, manager of clinical services for Phoenix Medical Management.
In the past, providers often dismissed trauma-induced outbursts as bad behavior or a character flaw. However, there’s a growing recognition that these responses are not only a predictable reaction to traumatic events but also preventable and manageable with the right approach.
Training staff members in Trauma-Informed Care (TIC), a patient-centered communication approach, can improve care, follow-up, and outcomes, and avoid exacerbating the problem, according to Wolfinger.
The impact of trauma
Many people think that trauma occurs in the wake of physical violence. However, a range of harmful experiences can traumatize patients, including accidents, natural disasters, serious or chronic illnesses, emotional abuse, neglect, racism or other forms of discrimination. Experts use the three E’s formula to understand how these experiences have affected patients, Wolfinger said. These are the Event, how the patient Experienced it, and its long-term Effect on them.
Research has shown that traumatic events can leave a lasting mark on people’s health. Adverse Childhood Experiences (ACES), for example, confer a higher risk of chronic illnesses, such as heart disease, depression, or substance use disorders. A hospital visit can exacerbate the problem, Wolfinger said, which is where TIC comes in. The model trains medical staff members to spot signs and symptoms of a trauma response and provide needed support without making the patient’s condition worse.
TIC is based on six guiding principles, according to the Substance Abuse and Mental Health Services Administration (SAMHSA):
Safety
Trustworthiness and transparency
Peer support
Collaboration and mutuality
Empowerment and choice
Cultural, historical, and gender sensitivity
Nowhere is this training more critical than in the ED, where emotions already run high. Many patients who come into the ED have experienced trauma in the past. Often those who’ve experienced childhood trauma avoid the doctor’s office and only seek care when it becomes an emergency.
Barriers to Implementation
While using TIC can be effective, many doctors aren’t familiar with the approach or even aware of how many of their patients have a trauma history. One survey found that only 16% of doctors believed that half of their patients had experienced trauma. Traditional constraints, such as a lack of time and resources, can also hinder TIC programs. Many hospitals are short-staffed, the workload is unrelenting, and burnout rates are high. Adding additional training and responsibilities is seen as an extra hurdle to overcome, Wolfinger said. However, organizations that invest the time can reap benefits, including improved safety for the care providers.
An effective TIC program starts with training on how to provide trauma-sensitive care and to de-escalate tense situations with stressed patients. It also implements screening procedures to flag patients in need of additional support and strives to improve the medical environment for patients. These include strategies such as increasing patient privacy, offering them more control over decision-making, and avoiding unnecessary physical contact.
“In my role as a trauma therapist in the emergency department, I’ve seen how medical exams can trigger severe trauma responses in patients. For example, I often write advocacy letters requesting modified physical exams for individuals with PTSD,” Wolfinger said. “These letters typically request accommodations such as allowing the patient to remain clothed, having a female provider present, and narrating care before physical contact. These small changes can dramatically reduce distress and prevent re-traumatization.”
Other procedural changes reduce the need for the patient to repeat upsetting details.
“Another example from the ED involves survivors of human trafficking. When multiple agencies are involved, we work to minimize how often the individual has to repeat their story,” Wolfinger said. “Coordinating between departments ensures that care is not only trauma-informed but also efficient and respectful, reducing both emotional and procedural harm.”
Case managers should also strive to match patients who will need additional support after discharge with community organizations and programs in addition to providing strong advocacy throughout the process.
“Whether I’m supporting a survivor of human trafficking or writing a letter to request a modified physical exam, my role is about advocacy. Trauma-informed care isn’t a luxury. It's a necessity for dignity and safety in medical care,” Wolfinger said.
Case Management Corner is your go-to source for insightful discussions on relevant topics in case management. Through an engaging interview-style format, our team members share their expertise, experiences, and best practices to keep you informed and empowered. Whether you're looking for industry updates, practical strategies, or real-world perspectives, we bring you valuable conversations designed to enhance your knowledge and support your professional growth. Stay tuned for expert insights straight from the field! Kelly Bilodeau has been a longtime writer for HCPro’s Case Management Monthly.

Evolution of Case Management: Moving Beyond the Triad Model
Today, the complexity of patient care, increasing patient volumes and the need for streamlined care transitions require a revised approach.
By Tiffany Ferguson, LMSW, CMAC, ACM
Note: This article appears on CMSAtoday’s website at CMSA Today (CMSQ) - Issue 4, 2025 - The Evolution of Hospital Case Management: Moving Beyond the Triad Model.
Hospital case management programs have long relied on the triad model, a structure that includes nurse case managers, social workers and utilization review specialists. While this model served a clear purpose in the late 1990s and early to mid-2000s, changes in healthcare demands, hospital throughput challenges and technological advancements have made it less effective. Today, the complexity of patient care, increasing patient volumes and the need for streamlined care transitions require a revised approach. Many hospitals across the country are feeling the impact of this shift, as the traditional structure no longer aligns with the demands of current patient and hospital needs and limited staffing resources.
Some programs have already begun to evolve beyond the triad model but have yet to clearly define or brand this new approach. Enter the Adaptive Model: a post-COVID framework that recognizes the staffing changes, the importance of social determinants of health, our mental health crisis and the needs of an aging baby boomer population. This model acknowledges that patients are simultaneously socially and medically complex. The Adaptive Model integrates non-licensed professionals as key team members, leverages technological advancements and expands the focus from unit-based inpatient care management to emergency department (ED), pre-surgical and hospitalized outpatient populations. It also marks the movement of utilization review from the traditional case management structure to a revenue cycle framework, deserving its own place on the professional stage.
The triad model was designed to optimize patient care by coordinating medical, social and financial aspects of a patient’s hospital stay. In this model, the nurse case manager focuses on discharge planning, the social worker provides psychosocial support and the utilization review specialist (typically a nurse) ensures medical necessity and appropriate resource utilization. Although these are vital and imperative concepts, there are several inefficiencies that have emerged in the siloing of these functions in today’s current landscape. The most significant issue is redundancy and role overlap, which creates confusion between the demands for the case manager versus the professional licensure that one holds in the current employment marketplace. It is common practice now to see nurse case managers and social workers performing the same role and simply "splitting the unit" as the functions of case management in the acute care setting require a divide and tackle approach to address patient progression of care. The triad model, while historically effective, has several inherent limitations:
Redundancy and Role Overlap: Case managers, social workers and utilization review specialists often perform overlapping tasks, leading to inefficiencies in discharge planning and communication. This fragmentation causes confusion among patients and providers about the roles of different team members.
Unit-Based Structure Limitations: The traditional model prioritizes inpatient hospitalized patients. This approach fails to address the increasing number of patients who require complex transitional planning before formal hospitalization or surgery.
Failure to Recognize the Physician Advisor(s): Although physician advisors were not formally recognized until after the triad model was established, their oversight and function to the team has changed the programmatic design for the care management model. Physician advisors may have dynamic roles with utilization review, documentation integrity and addressing continued stays that are not medically necessary.
Limited Use of Non-Licensed Professionals: Similarly, the model fails to recognize the expansion of job functions to non-licensed professionals. The model hinders the evolved ability for professionals to work top of license due to the logistical demands of the role, reducing the time they can spend on high-value patient interactions.
Inadequate Technology Utilization: The model was created before the advancement of post-acute platforms, machine learning and automation. Many of the functions that require manual chart review can be more efficiently performed through technology support systems, changing the role for non-licensed and licensed team members.
Insufficient Focus on Patient Throughput: Although originally designed to support patient progression of care, the triad model was designed from a unit-based case management perspective. With rising emergency department volumes and an increasing emphasis on outpatient care, hospitals now require a model that emphasizes proactive care coordination before inpatient admission and well after the patient hospitalization under a more value-based/ population health structure.
Social Determinants and Patient Complexity: With new social determinants of health (SDoH) requirements and the rise of patient social complexity leading to greater social admissions, case management departments are forced to evolve and develop creative roles and specialized roles for social workers to tackle this population. Through time, this has also led to expansion of specialized case management roles for unique hospital populations such as palliative, oncology and obstetrics, to name a few.
The Shift of Utilization Review to Revenue Cycle: Utilization review (UR) has increasingly moved out of the case management structure, depending on hospital size, as its own program as a result of payer demands and a stronger focus on medical necessity and denials prevention. This greater alignment with revenue cycle does create some shifts for the traditional case management model, as many utilization review nurses are working remotely, handing some of the functions back to the case managers. This change, likely an article on its own, means utilization review is also changing away from a unit-based model to a functional model to evaluate patients across review and payer needs, leveraging technology for greater workflow efficiency.
The Adaptive Case Management Model
To address these inefficiencies, hospital case management must recognize the already in motion transition to a model that prioritizes:
The Inclusion of Non-Licensed Professionals
A Staffing Structure Focused on Technology and Skilled Communication
A Shift Away from Unit-Based Case Management
A key component of the new model is the strategic use of non-licensed professionals, such as case management assistants, patient navigators, care coordinators, community health workers, etc. These individuals are integral to the success of case management departments and require their own training and professional support to acknowledge the vital role they are serving to facilitate care transitions and support post-acute care services (McLoughlin-Davis, 2019). These individuals range from high school education, the patient care technicians, to associate and bachelor’s degree professionals who can support a wide variety of functions in the case management department. Now more than ever, these individuals are filling gaps in case management programs to address significant nursing shortages across the country. Some of the important services they provide include but are not limited to:
Scheduling follow-up appointments
Coordinating durable medical equipment (DME) and home health services
Arranging transportation
Completing insurance and financial paperwork
Following up on post-emergency room and post-acute referrals
Coordinating outpatient care services
Providing resources for social determinants of health
Delivering regulatory notices
Research has shown that leveraging non-licensed staff in discharge planning improves efficiency and allows licensed professionals to focus on clinical decision-making. By integrating this workforce, hospitals have significantly improved discharge times and reduced readmission rates (AHRQ, 2021).
The Adaptive Model recognizes the requirement for technology to enhance case management efficiency. Some of the key technological advancements now include automated workflows, telehealth and optimization of our electronic medical records. AI-driven case management software can help identify patients needing case management intervention earlier in their hospital stay (Garrett, 2024). Virtual discharge planning and follow-up visits improve post-discharge care coordination. Standardized documentation and decision-support tools improve communication among case management teams.
By leveraging these technologies, the role of case managers, whether nurses or social workers, becomes more focused on high-value clinical decision-making, while non-licensed staff and technology handle many of the administrative tasks. The model also shifts away from tenure as a measure of success, instead requiring a workforce with strong communication, technology and problem-solving skills to facilitate better interactions with medical teams, patients and outpatient providers.
Instead of adhering to traditional unit-based case management, the Adaptive Model acknowledges and prioritizes patients in the ED for early intervention to prevent unnecessary admissions and expedite appropriate discharges out of the emergency room. It also acknowledges the growing number of hospitalized outpatients, including surgical patients and those under observation. Case management in the Adaptive Model begins before the patient enters the hospital, with pre-operative assessments, education and planning.
Additionally, the Adaptive Model recognizes the increasing social complexity of patients. This has evolved from a singular social work function, to care teams equipped to handle these complexities through comprehensive, multidisciplinary approaches that adapt to the local community.
The traditional triad model of hospital case management is no longer sufficient in today’s fast-paced healthcare environment. The Adaptive Model provides flexibility to the local landscape and the transformative nature of healthcare. The model encompasses disciplines outside nurses and social workers as integral to the case management team such as non-licensed professionals, physician advisors and pre or post hospital case management roles. The Adaptive Model requires a new workforce with strong communication skills and technology acumen who can leverage the fast-paced technological advancements currently on the horizon in the case management space. Finally, the model expands the focus outside inpatients to encompass independent staffing structures for emergencies, pre-surgical, bedded outpatients and post-discharge outpatient settings. The Adaptive Model leans into the change for utilization review from one part of the three-legged stool to its own specialized set of professionals deeply tied to the clinical revenue cycle team members, thus shifting some of the requirements back to the case management team members. As healthcare continues to evolve, the Adaptive Model offers a pathway to a more efficient, patient-centered case management approach.

Case Management Corner: Avoiding Common Short-Stay Audit Pitfalls
Medicare short-stay review errors often occur because the staff responsible for the process aren’t given clear guidance.
By Kelly Bilodeau
Traditional Medicare short-stay inpatient stay audits help ensure appropriate patient status decisions and accurate billing. However, organizations commonly struggle to implement a compliant process and run afoul of Medicare regulations, said Sara Williams, MSN, RN, ACM-RN, vice president of clinical strategy at Phoenix.
“Many facilities I’ve visited lately have gaps in their Medicare short-stay audit process,” she said. Hospitals often allow nurses to make downgrade determinations for patient cases that don’t meet one of the Medicare exclusions for an inpatient stay that lasts less than two midnights. However, CMS regulations reserve this role for a physician member of the UR committee. “Other organizations weren’t notifying patients within 48 hours that their stay would be billed under their Part B benefit instead of Part A after a review found they didn’t qualify for an inpatient admission,” Williams said. “Most of the organizations weren’t notifying the patient at all. They were just making the change to Part B billing.”
Monitoring compliance
CMS expects facilities to classify patients accurately, and short-stay reviews are a simple way to verify that the patient’s status is correct. “Medicare does audit these short stays,” Williams said. The annual Program for Evaluating Payment Patterns Electronic Report (PEPPER) provides valuable insights into an organization’s one-day stay trends, comparing them to national and state data. It also allows facilities to compare themselves against organizations in similar locations. So, facilities should familiarize themselves with the information contained in the report.
CMS allows for short-stay exceptions, so a UR nurse may determine that a case meets inpatient criteria even if it falls short of the required two midnights. For example, the stay may qualify under an exclusion if the patient’s surgical procedure is on the inpatient-only list. Some other examples of exclusions include the following:
· The patient expired before the second midnight.
· The patient was transferred to a higher level of care.
· The patient transferred from another facility and has two medically necessary midnights combined between the two hospital stays.
· The patient left the facility against medical advice.
· The patient transitioned to hospice during an appropriate inpatient hospitalization.
However, if the case doesn’t meet a defined exclusion, a physician member of the UM committee must review it to make a final determination, Williams said. If the UM Committee physician determines the case doesn’t meet the requirements for Part A billing, they must notify the attending provider and give them a chance to weigh in. The attending can respond within a set time frame to affirm the change, or choose not to respond, which is also seen as an affirmation. In these cases, the hospital must self-deny the original Part A claim and rebill the claim under Part B. This change triggers a mandatory patient notification. “The letter that goes to the patient needs to be very succinct and explain the billing change because it can be confusing. I've seen patients call and say: I was in the hospital? Why are you saying that's not covered?’” Williams said.
However, if the attending physician disagrees with the UM Committee physician’s assessment, they can submit additional details and the case will move to a second review by another physician member of the UM Committee who makes the final determination.
Setting up supportive systems
Medicare short-stay review errors often occur because the staff responsible for the process aren’t given clear guidance, and due to confusion about the requirements outlined in the Medicare Utilization Review Conditions of Participation, Williams said. Providing additional education and tools for UR nurses and UM Committee physicians who carry out these reviews can often solve the problem.
Organizations should establish workflows to support the process, including communication channels with revenue cycle staff members to bill corrected claims accurately. “Leverage your EMR as much as you can to automate this process,” Williams said.
Although the Two-Midnight Rule went into effect more than a decade ago, organizations still struggle to understand the complexities of the short-stay review process. Proper documentation can help. Providers should clearly document why a two-midnight stay in the hospital is medically necessary for each inpatient. Avoid canned, check-box responses. “In addition, if the patient does get better more quickly than expected, there's very clear documentation on the back end to say that,” Williams said. “Sometimes you may anticipate that a patient is going to be hospitalized for two midnights or more, and they improve more quickly than expected,” Williams said.
Establishing a proactive process and coordination between UR and Revenue Cycle/Integrity departments can help ensure your organization gets it right.
Case Management Corner is your go-to source for insightful discussions on relevant topics in case management. Through an engaging interview-style format, our team members share their expertise, experiences, and best practices to keep you informed and empowered. Whether you're looking for industry updates, practical strategies, or real-world perspectives, we bring you valuable conversations designed to enhance your knowledge and support your professional growth. Stay tuned for expert insights straight from the field! Kelly Bilodeau has been a longtime writer for HCPro’s Case Management Monthly.

Could UnitedHealth Group’s Woes Ultimately Result in Improvements?
Despite multiple lawsuits and threatened actions by private, state, and federal agencies across the country, UHG has been a longtime dominant force related to revenue cycle, provider staffing, utilization, and managed and commercial health insurance plans.
By Juliet Ugarte Hopkins, MD, ACPA-C
In the last seven months, UnitedHealth Group (UHG) has been racked by devastating events, from the massive cyberattack on Change Healthcare in October to the murder of UnitedHealthcare’s (UHC’s) CEO, Brian Thompson, in December.
At the end of last month, after reporting a weaker-than-expected first quarter (despite posting $6.3 billion in profit during the same timeframe), UHG stock plummeted by more than 22 percent, faster than any drop seen by the company in the last 25 years.
UHG’s CEO at the time, Andrew Witty, associated the poor performance with beneficiaries – especially those within their Medicare Advantage (MA) plans – utilizing more medical services than expected. This comment truly (and possibly, inadvertently) illustrated the point that health insurance companies make more money for their shareholders when their beneficiaries don’t seek out or receive healthcare services.
This comes as no surprise to case managers everywhere who try and secure skilled nursing facility (SNF) or inpatient rehabilitation facility (IRF) care for hospitalized patients and repetitively face stalling tactics (and ultimately, denials).
Then, on May 13, UHG stock dropped again, this time by more than 16 percent, in the hours after Witty abruptly resigned “for personal reasons.” Despite multiple lawsuits and threatened actions by private, state, and federal agencies across the country, UHG has been a longtime dominant force related to revenue cycle, provider staffing, utilization, and managed and commercial health insurance plans.
The owner of Aetna, CVS Health, as well as Humana have also seen recent declines in their profitability, but to a lesser extent than that of UHG. This is likely a reflection of what historically has served UHG so well in the past – a profound presence in healthcare across the country.
Last year alone, UHG acquired or created over 250 subsidiaries, including acute surgery centers, home care companies, and pharmacies. The thousands and thousands of new beneficiaries that came along with these subsidiaries – many of whom are covered by UHC’s managed Medicare plans – possibly led to the unanticipated increase in costs of medical services.
On May 15, UHG stock plunged yet again, by more than 15 percent, after the Wall Street Journal reported the U.S. Department of Justice (DOJ) has been conducting a criminal investigation since last summer into possible Medicare fraud carried out by UHG’s Medicare Advantage arm of the business. This is in addition to a DOJ civil investigation announced at the start of the year, looking into the possibility of UHG inappropriately assigning more significant diagnoses to beneficiaries to obtain larger or extra payments from Medicare.
While an official announcement from the DOJ has not yet been made, considering that UHG stock is down almost 50 percent since the start of 2025 and has lost over $300 billion of its $600 billion market value in one month, it’s clear recent events have taken their toll on the company and are not a simple blip on the radar. Since the road toward the astronomical profitability UHG has enjoyed in prior years was paved with narrow medical care access for beneficiaries, what could these recent events mean for hospitals and the patients they serve? Increased scrutiny of the medical necessity of emergency department care or hospitalizations? Escalated denials related to out-of-hospital continuation of care at SNFs, access to home nursing and therapy services, or coverage of medications and durable medical equipment (DME)?
Unfortunately, it’s very possible that beneficiaries and the health systems serving them will experience most of these frustrations.
On the other hand, should hospitals dare to dream that positive changes are on the horizon, concerning their dealings with UHC? In an effort of good faith, might UHC throttle back their aggressive tactics, involving an overwhelm-and-overcome strategy related to denials, and put less emphasis on shareholder dividends and more on patient care?
While a possibility, it appears less likely now, given that Witty was quickly replaced by former UHG CEO Stephen Hemsley, who ran the organization from 2006–2017.
References:
What UnitedHealth’s Stock Drop Reveals About Medicare Advantage, N. Adam Brown, MD, MBA, MedPage Today, April 29, 2025
UnitedHealth Group Reports Third Quarter 2024 Results, BusinessWire, October 15, 2024
UnitedHealthcare stock takes massive hit after earning forecast cut, Fox 9 KMSP and Associated Press, April 17, 2025
UnitedHealth Group stock tumbles; Andrew Witty steps down as group CEO, Martin Baccardax, The Street, May 13, 2025
UnitedHealth Group shares plunge 13% on report of DOJ probe into possible Medicare fraud, Annika Kim Constantino, CNBC, May 15, 2025
UnitedHealth Responds to Fraud Investigation Report: ‘Deeply Irresponsible’, Newsweek, May 15, 2025

Navigating the Two-Midnight Rule with Medicare Advantage
Despite the gains that many hospitals felt regarding MA final rule 4201, this appears to be an interesting clarification regarding the difference between the two-midnight presumption verse the two-midnight benchmark.
By Tiffany Ferguson, LMSW, CMAC, ACM
In its Contract Year 2026 Medicare Advantage and Part D Final Rule (CMS-4208-F), the Centers for Medicare & Medicaid Services (CMS) addressed ongoing confusion about how Medicare Advantage (MA) plans apply inpatient criteria, specifically the “two-midnight rule” and how this interacts with appeal processes through the Independent Review Entity (IRE).
Layered deep in the seventh provision to clarify terminology regarding inpatient level of care, which primarily surrounds clarification of concurrent status changes and notice requirements for MA plans to patients, you will find a question from a key commenter who raised concerns about the disconnect between the two-midnight presumption used in traditional Medicare and the flexibility afforded to MA plans in denying inpatient claims.
The concern focused on the patient experience: beneficiaries are often admitted under an inpatient order, only to learn later that their stay has been reclassified as outpatient or observation, despite receiving the same level of hospital care. This results in potential financial liability and confusion, particularly when coverage status changes mid-stay.
Despite the gains that many hospitals felt regarding MA final rule 4201, this appears to be an interesting clarification regarding the difference between the two-midnight presumption verse the two-midnight benchmark.
CMS clarified that while the rule strengthens various enrollee protections, it does not extend the two-midnight presumption to MA plans. The presumption, which deems inpatient admissions crossing two midnights as appropriate for Part A payment, was designed as a safeguard for traditional Medicare post-payment reviews conducted by Recovery Audit Contractors (RACs) or Quality Improvement Organizations (QIOs). The response then went on to say that this ruling is not a universal standard and does not bind MA organizations.
MA plans, however, are required to follow the inpatient admission criteria outlined in 42 CFR §412.3, commonly referred to as the “two-midnight benchmark.” This means that if a physician expects the patient to require hospital care spanning at least two midnights and formally admits the patient as such, the criteria for inpatient coverage may be met assuming the documentation supports medical necessity.
Importantly, CMS emphasized that if the IRE overturns an MA denial and determines that the inpatient admission meets criteria under §412.3, MA plans must honor the IRE’s decision and effectuate payment.
Although the two-midnight presumption remains outside the MA scope, CMS has taken other steps in the final rule to reduce patient and provider burden. These include stronger notice requirements for communication tools from MA plans to ensure level of care changes are communicated timely to patients, clarification on when MA beneficiary financial liability is triggered, and limitations on retroactive reclassification of previously approved inpatient stays.
To safeguard against the two-midnight benchmarking allowance for MA plans, the burden of proof will remain on providers to ensure thorough documentation surrounding intentions for admission, and the clinical rationale for inpatient care.