

Kepro rebranding As Acentra Health
Kepro rebranding in Fall 2024
Sometime this fall, Kepro will be known as Acentra Health.
During this rebrand, case reviews and all other services will continue without interruption. Providers will be encouraged to update their beneficiary notices – the Important Message from Medicare (IM) and the Notice of Medicare Non-Coverage (NOMNC) – by replacing "Kepro" with "Acentra Health." However, notices with the QIO name of “Kepro” listed will still be accepted and validated.
For ongoing updates about Kepro’s name change and the impact it has on Medicare providers, stakeholders, and beneficiaries, visit www.keproqio.com/acentrahealth. It is anticipated that the transition to Acentra Health will be complete by Fall 2024.

Major Healthcare Initiatives Get Presidential Push
Overall, these investments align with the Administration’s goals of improving healthcare access, addressing mental health challenges, and ensuring equitable care for all Americans.
By Tiffany Ferguson, LMSW, CMAC, ACM
In March the Biden-Harris Administration submitted their budget proposal for the Health Resources and Services Administration (HRSA) for the 2025 fiscal year, which outlines several key investments to tackle their top healthcare initiatives. These include the following:
Youth Mental Health Crisis: There have been several disturbing trends emerge in the area of youth mental health, with nearly one-third of youths reporting experiences with poor mental health and 1 in 5 students reporting seriously considering suicide. The budget focuses on expanding access to mental health and substance use disorder treatment. Investments include training 12,000 new behavioral health providers, creating a peer-to-peer mental health support program for youths, supporting mental health training for pediatricians, and integrating mental health services into community health centers.
Maternity Care Deserts: To address the lack of maternity care services in certain areas, the budget invests in building obstetric capacity in underserved areas, training more labor and delivery nurses and certified nurse midwives, establishing a community-based doula workforce, and expanding access to maternal mental health support through the National Maternal Mental Health Hotline at 1-833-TLC-MAMA.
Closing Gaps in Access to Primary Care: The Administration has indicated that it recognizes the barriers to accessing primary care, such as lack of providers, lack of access to transportation, and limited availability in appointment times and provider hours; this is only exacerbated in rural and underserved communities. The budget aims to double the federal investment in community health centers, expand health center street medicine services for the homeless, and extend health center operating hours.
Meeting Opioid Treatment and Recovery Needs: Given the challenges in rural communities regarding opioid use disorder treatment, the budget focuses on creating more access to treatment, supporting mobile units for medication-assisted treatment, integrating support services, and expanding the rural substance use disorder workforce.
Growing the Healthcare Workforce: Addressing projected shortages in healthcare occupations, the budget provides scholarships and loan repayment programs to over 24,000 clinicians, nurses, and healthcare professionals to provide services in underserved areas. The budget will also be supporting more than 1,800 medical and dental residents to work and train in rural communities, and funds new approaches to recruit and diversify the healthcare workforce.
Transforming the Organ Matching System: To enhance the organ procurement and transplantation system, the budget doubles funding for the system, aims to increase competition, and supports updates to improve performance and innovation.
Overall, these investments align with the Administration’s goals of improving healthcare access, addressing mental health challenges, and ensuring equitable care for all Americans.

Understanding the Connection Between Observation Rate & CMI
Metrics like observation rate, denials rate, and case mix index (CMI), although interconnected, are frequently established with independent goals, further complicating the pursuit of comprehensive success.
By Tiffany Ferguson, LMSW, CMAC, ACM
EDITOR’S NOTE: The context for this article was conceptualized from a recent ACPA Town Hall meeting on observation metrics and a presentation by the author and Dr. Mohla at NPAC 2024 on observation metrics. Also used as a reference was the ACDIS white paper “Demystifying and Communicating Case-Mix Index,” published in 2022.
Those in healthcare roles frequently experience the stress associated with meeting key performance indicators (KPIs) compared to benchmark standards. While achieving these goals can be gratifying, there are instances when they can seem unattainable, often due to the arbitrary nature of how the metrics are set, relying on external benchmarks or ambitious targets without a comprehensive review of processes and data. Metrics like observation rate, denials rate, and case mix index (CMI), although interconnected, are frequently established with independent goals, further complicating the pursuit of comprehensive success.
Utilization management (UM) has long grappled with a historical bias, perceiving observation as unfavorable while favoring inpatient care for financial security – an orientation reflected in the overarching objective of hospitals and departments to “lower the observation rate.” While there may be valid opportunities to reduce the observation rate, it is crucial to carefully consider internal processes and target needs before establishing an ideal or benchmarked lower limits.
Simultaneously, clinical documentation improvement (CDI) aims to accurately capture patient acuity, with benchmark objectives to achieve higher-weighted DRG classifications, resulting in a higher CMI for the hospital. Both objectives are financially significant and encouraged by hospital leaders, particularly in a fee-for-service environment.
However, they can be at odds; aggressively reducing the observation rate might prompt a shift towards designating more cases as inpatient care, leading to a higher proportion of lower-weighted DRG patients for CDI review and lowering the hospital’s CMI. Although the observation rate may decrease, so would the CMI.
This practice could also lead to an increase in post-discharge W2s and payer denials, potentially increasing accounts receivable (A/R) days and denial recovery, thus negatively impacting the financial goals for your revenue cycle and business office. It is plausible that cases initially pushed towards inpatient care, when observation might have been more appropriate, could eventually result in payment at the outpatient rate, often less than if observation was ordered properly at the outset, during the appeals process.
This lower-than-expected reimbursement would then hide in the patient accounting world, while the reported observation rate would remain low.
On the flip side, adopting an excessively conservative approach in determining level of care to preempt payer denials could lead to a situation in which more patients are retained in outpatient status with observation services, driven by apprehension of payer resistance. In this context, although the observation rate might be higher, the CMI could also rise, given that only patients unequivocally confirmed for inpatient care contribute to this metric. While denials may decrease, this cautious strategy carries the inherent risk of establishing a reimbursement structure that limits potential level-of-care opportunities for inpatient designation, despite the medical treatment delivered or clinical guidelines. Striking the right balance is not easy, but it is crucial to avoid the unintended consequence of limiting revenue for the sake of an overly conservative stance on care-level designations.
Determining level of care should by prioritized by doing what is right for the patient, considering factors such as medical necessity, patient acuity, and medical decision-making, rather than the pressures of meeting arbitrary benchmarks, which are often based on data from hospitals whose demographics and offerings are in distinct contrast to a hospital’s own.
Finding hospitals with similar patient populations, services, and physician behavior can allow developing appropriate benchmarks, which then could serve as a barometer to ensure that a health system aligns reasonably with their peers, rather than the sole driving force being operational efficiency.
Instead, consider a focus on understanding how data is collected and analyzed, with a collective goal that assesses hospital processes and performance opportunities across utilization management, CDI, and the denials/appeals team.

White House Makes Additional $1.7 Billion Investment In Health
These commitments collectively contribute to demonstrate comprehensive efforts and offer tangible solutions to tackle hunger, improve nutrition, and reduce health disparities.
By Tiffany Ferguson, LMSW, CMAC, ACM
The Biden-Harris Administration has unveiled 141 new commitments from diverse stakeholders nationwide as part of the White House Challenge to End Hunger and Build Healthy Communities.
Such stakeholders include health systems, insurers, companies, nonprofits, philanthropic groups, academic institutions, and local elected officials. Second Gentleman Douglas Emhoff announced these commitments alongside key figures like White House Domestic Policy Advisor Neera Tanden, Agriculture Secretary Tom Vilsack, and the Chairs of the President’s Council on Sports, Fitness, and Nutrition: chef José Andrés and basketball player Elena Delle Donne.
This Challenge is aligned with President Biden’s goal to end hunger and reduce diet-related diseases by 2030, while also addressing health disparities. The $1.7 billion in new commitments announced build upon the $8 billion commitments made at the White House Conference on Hunger, Nutrition, and Health in September 2022. These efforts complement the National Strategy on Hunger, Nutrition, and Health, with commitments cultivated in collaboration with the Centers for Disease Control and Prevention (CDC) Foundation.
One significant aspect of the commitments is the partnership between major sports leagues, players’ associations, and the President’s Council on Sports, Fitness, and Nutrition, which aims to boost physical activity and increase nutrition programming across the country. Fourteen sports leagues and players’ associations have committed to expanding access to physical activity and promoting healthy lifestyles.
Various commitments were announced, ranging from the Harlem Globetrotters’ public awareness campaign on nutrition and physical activity in cities like Cleveland, Baton Rouge, and Seattle, which also includes the launches of task forces to end hunger and reduce diet-related diseases. Companies such as Ahold Delhaize USA have committed almost $1 million for nutrition education for children, while health systems like Ascension are focusing on addressing the social determinants of health (SDoH) through a closed-loop referral process and providing hospital-based produce markets in 100 percent of their sites of care (that is, 139 hospitals across 19 states).
Other commitments include Blue Cross Blue Shield of North Carolina expanding nutrition coaching and healthy food delivery, Food Forward providing access to 290 million pounds of fresh produce to distribute to those facing food insecurity, and the Gaples Institute offering nutrition education resources to 100 additional U.S. medical schools.
Highmark Health and Allegheny Health Network will mobilize over $30 million through 2030 to conduct assessments, expand Healthy Food Centers, and address non-medical barriers to health. Homeplate Solutions, through an artificial intelligence (AI)-enabled technology platform, aims to provide greater affordability and accessibility to food for community-based nutrition providers.
The National Association of Chronic Disease Directors has committed $2 million to improve physical activity and nutrition, and to reduce chronic and diet-related diseases, through various programs across states and school districts.
The National Strategy underscores the Administration’s whole-of-government approach, with actions including U.S. Department of Agriculture (USDA) investments in school meal programs, the Food and Drug Administration’s (FDA’s) study on a front-of-package system for food packages, and U.S. Department of Health and Human Services (HHS) initiatives to address the SDoH under Medicaid and the Children’s Health Insurance Program (CHIP). This initiative directly compliments the SDoH food insecurity domain for questions in the outpatient and inpatient settings. These commitments collectively contribute to demonstrate comprehensive efforts and offer tangible solutions to tackle hunger, improve nutrition, and reduce health disparities.
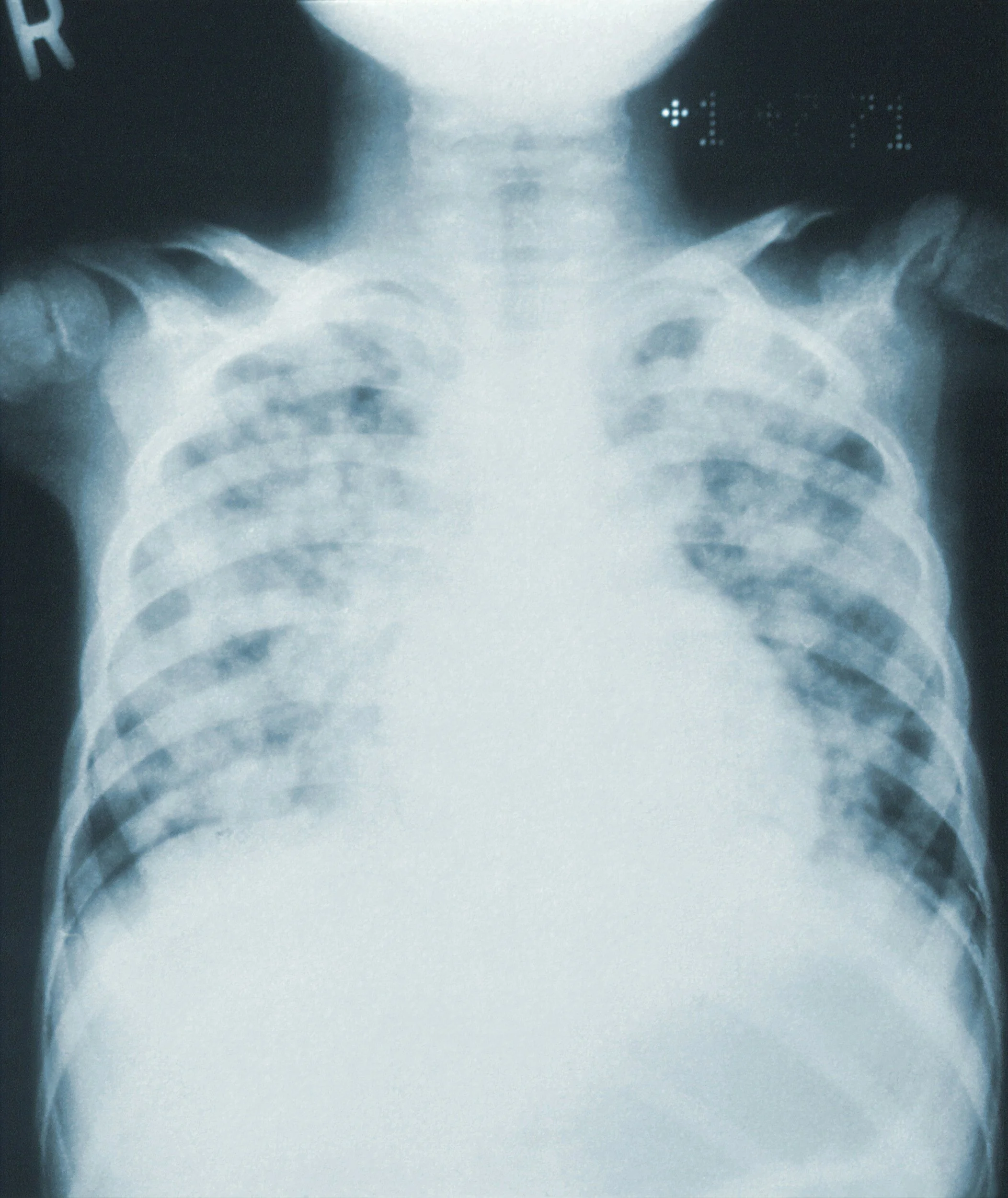
How to Prevent Pneumonia DRG Denials
Make sure clinical documentation integrity specialists are vigilant when reviewing records of patients with pneumonia, and query when indicated.
By Erica E. Remer, MD, CCDS
When I ask facilities what their most common denials are, invariably, pneumonia makes the list. That was my personal experience when I handled clinical validation denials as a physician advisor. Most of them I deemed appropriate denials and declined to appeal. Recently, I’ve been working on a project where I’ve been assessing encounters resulting in DRG (Diagnosis-Related Group) downgrades, and I would like to specifically address pneumonia today.
The typical scenario is a patient with underlying comorbidities of heart failure or chronic obstructive pulmonary disease (COPD) and presents to the emergency department complaining of shortness of breath and cough. The patient may have no or low-grade fever. The chest X-ray is not compelling – no distinct infiltrate is seen. The radiologist may be hedgy, noting markings that “could be pneumonitis or pulmonary edema or atelectasis; clinical correlation necessary.”
The emergency physician or hospitalist empirically treats for pneumonia and makes an uncertain diagnosis (e.g., possible, probable, likely). The issue arises when the condition is neither definitively ruled in, during the course of the encounter nor conclusively ruled out. The uncertain diagnosis is propagated through copying and pasting. There are also concomitant issues, with hypoxia being labeled acute hypoxic respiratory failure, or sepsis being diagnosed without evidence of organ dysfunction.
As a reviewer, I am able to take in the entire admission through the lens of the retro-spectoscope. At the end of the stay, it may be that much easier to ascertain that the entire clinical presentation was due to acute-on-chronic heart failure (HF) due to fluid overload (e.g., missed dialysis) or exacerbation of COPD from viral bronchitis. The definition of principal diagnosis, which establishes the DRG, is “that condition which, after study, was chiefly responsible for occasioning the admission of the patient to the hospital for care.” If I can tell that the derangement causing the hospitalization was the HF or COPD, and I doubt the validity of the pneumonia, so can the payor, and they will want to revise the DRG accordingly.
The initial providers are not going to know how the encounter is going to play out. It is reasonable to empirically treat for pneumonia. The error occurs when the subsequent providers fail to evolve, resolve, remove, and recap. The diagnosis should evolve as more information becomes available, like culture results. Resolving is documenting that the condition has been successfully managed and is no longer an active problem. “Remove” is what should be done when a condition has been ruled out. All clinically significant diagnoses should be recapped in the discharge summary to encapsulate the hospital course and tell the story of the encounter.
Elements that imperil the diagnosis of pneumonia are:
Lack of fever or elevated white blood cell count, normal vital signs; no evidence of the patient being in any respiratory distress, or appearing ill or toxic;
No infiltrate ever materializes on either chest X-ray or CT scan;
The provider hesitantly diagnoses pneumonia in the setting of organ dysfunction (e.g., metabolic encephalopathy, acute hypoxic respiratory failure, acute kidney injury, Type 2 myocardial infarction), but does not diagnose sepsis;
Consultants such as pulmonologist or infectious disease don’t make a diagnosis of pneumonia in the same patient with the same information;
The assessment and plan (A&P) is unchanging, and the diagnosis remains uncertain; and
Pneumonia is absent from the discharge summary.
Here is what the provider can do to prevent pneumonia denial jeopardy:
Paint the picture of a patient with pneumonia – providers should call out fever, tachypnea, increased shortness of breath, chest pain, and/or hypoxemia, and link the signs/symptoms with the pneumonia, especially if there are other pulmonary confounding diagnoses;
Rethink the diagnosis if there are no radiological findings suggestive of pneumonia. It is hard to sell pneumonia to a payor without an infiltrate;
As the encounter progresses in a patient with an uncertain diagnosis of pneumonia, either definitively rule in, rule out, or intentionally maintain uncertainty. Each day, you should have more information and data on which to base your diagnosis;
Link pneumonia with acute hypoxic respiratory failure or with sepsis if those diagnoses are concurrent. If pneumonia gets ruled out but the provider is retaining sepsis as a diagnosis, ensure there is an alternate infection as a source;
Consider the consultants’ opinions. Either agree and incorporate their diagnoses and specificity into your documentation, or disagree and document your rationale. Discuss it with them so everyone can be on the same page while taking care of the patient. Avert internal inconsistency;
If pneumonia is ruled out, document the reasoning, and declare it ruled out. The next day, pneumonia should no longer be on the impression list. Don’t just drop it without explanation. It will not be clear whether it was ruled out or just accidentally forgotten; and
The discharge summary should tell the story of the patient encounter. If they really had pneumonia, it should appear in the list of discharge diagnoses. If the course of antibiotics is not complete, prescribe it in the discharge instructions.
One of the most important things to do is to perform clinical validation prior to final coding and billing. Make sure clinical documentation integrity specialists are vigilant when reviewing records of patients with pneumonia, and query when indicated. It may not be feasible to do a mandatory review of all patients with pneumonia, but it may be possible to review all pneumonia from a specific provider who has a history of being lax at diagnosing it.
It is understandable, even desirable, to make the diagnosis of pneumonia preliminarily and have it ruled out over the course of the next few days. However, the provider needs to make sure their documentation tells the story of the patient encounter accurately. An ounce of prevention is worth hours of fighting clinical validation denials!

CDI Queries Work Best if the Recipient is Kept in Mind
When a CDIS composes a query, they should be providing the provider with the clinical indicators they need to make a thoughtful, informed decision.
By Erica E. Remer, MD, CCDS
I had an epiphany the other day while discussing compliant query composition with a very knowledgeable clinical documentation integrity specialist (CDIS). It will be easiest to explain if I share the original query first.
The following clinical indicators were noted in this patient’s medical record:
A 70-year-old female was admitted with sepsis, pyelonephritis, urinary tract infection, and documented “worsening altered mental status.” There was an infectious disease consult. The urine culture grew Klebsiella. The patient was treated with IV antibiotics.
Please clarify the patient’s altered mental status.
Based on these clinical indicators and your professional judgment, please document in the medical record whether you believe any of the following conditions are present:
Acute metabolic encephalopathy
Septic encephalopathy
Confusion only
AMS with no further specificity
Delirium
Other (specify)
Unable to determine
When a CDIS composes a query, they should be providing the provider with the clinical indicators they need to make a thoughtful, informed decision. The CDIS can pick and choose which clinical indicators to offer, but they should give both clinical indicators that support the condition they might be hoping to get in response AND clinical indicators that might not be consistent. The intent is to get the right answer, meaning the condition that is clinically valid and significant. The fact that a blood culture grew out streptococcus might be very pertinent in a clinical validation query regarding “probable gram-negative pneumonia.”
This was a made-up scenario, but other clinical indicators that might have been relevant could have been the results of blood cultures, information from a neurology consult, and whether the final mental status returned to baseline. And what did the discharge summary say?
Next, ensure that the question being asked is the question you want answered. In this case, the CDIS wants to know if the “altered mental status” could be categorized as some comorbid condition (not used in this context here as a CC or MCC), as opposed to a sign/symptom.
(As an aside, a symptom is a manifestation of a condition subjectively reported by the patient, whereas a sign is a manifestation which the provider objectively perceives, e.g., “felt feverish” versus T 39° Celsius)
The questions asked were: “Please clarify patient’s altered mental status” and do you “believe any of the following conditions were present?” The provider may think to himself/herself: saying “altered mental status” is pretty clear. The reader may disagree. Altered mental status could mean lots of things, including lethargy, confusion, or difficulty understanding or expressing oneself.
An alternate way to pose the query could have been, “Based on your clinical judgment, is there a more specific diagnosis that clarifies the patient’s altered mental status?”
We then honed in on the offered choices. My colleague felt we could eliminate “septic encephalopathy,” since it gets coded as metabolic encephalopathy anyway. This was emblematic of one of the key points of this article. Doctors don’t really do their documentation for coding. They do it for clinical communication. In fact, they probably don’t even know (or would particularly care) that “septic encephalopathy” is compliantly coded as “metabolic encephalopathy.”
But I wouldn’t remove that choice, because there may be providers who do use that terminology, and would feel it clarified the altered mental status. It also might serve as support for acute sepsis-related organ dysfunction (establishing sepsis). So, I would leave two choices that get coded the same way. I want the verbiage to feel authentic, in their voice.
I would also remove the “acute” from “acute metabolic encephalopathy.” I don’t want to leave words in choices that might make a clinician hesitate or scratch their head. What if they felt it had developed over two or three days and they really thought it was “subacute.” Would offering a choice with “acute” in it stymie them?
If the provider had described the altered mental status as “confusion” somewhere, then “confusion only” would be acceptable (even if it is undesirable!). If they had not, I would not potentially put those words in the provider’s mouth.
I also wouldn’t use “AMS” in a choice because I can’t compliantly index that to R41.82, Altered mental status, unspecified. I wouldn’t use an initialism here; I would type out “altered mental status.”
Another aside (from the CDC):
Abbreviation: truncated word; e.g., “min” for minutes
Acronym: made up of parts of phrases it stands for and pronounced as a word; e.g., SIRS for Systemic Inflammatory Response Syndrome
Initialism: Similar to acronym, but pronounced by enunciating each letter; e.g., SOB for shortness of breath
What about delirium? Should we introduce a new condition that wasn’t mentioned in the record? It depends. Is it consistent with the clinical indicators? If the nurses or different providers mentioned waxing and waning attention or a fluctuating course, I would present that in my clinical indicators and then offer that a selection of “delirium” would not be inappropriate.
Lastly, I HATE “unable to determine” as a choice in multiple-choice queries. If you give an “other” or free-text option, you don’t need to use “unable to determine.” It is appropriate and “required” in POA and yes/no queries, per the Compliant Query Practice Brief. I don’t like setting myself up for the provider choosing an option that is uncodable, sets up more questions, or is not clarifying.
My advice is to make sure that every query is for a purpose (to clarify the record and make it as accurate and specific as possible) and ensure that it is understandable by the clinician. It doesn’t help the CDIS’s metrics and productivity to generate a query if it just confounds the provider and doesn’t result in a useful response.

New Outpatient SDoH Codes: How they Apply and What Can be Done
Almost two months into the 2024 Outpatient Prospective Payment System (OPPS), I thought I would provide some clarity regarding the new social determinants of health (SDoH) and supportive service codes that have been released – specifically, the SDoH assessment, community health integration, and principal illness integration.
By Tiffany Ferguson, LMSW, CMAC, ACM
I thought I would provide some clarity regarding the new social determinants of health (SDoH) and supportive service codes that have been released in the 2024 Outpatient Prospective Payment System (OPPS) – specifically, the SDoH assessment, community health integration, and principal illness integration. This article was prompted after some questions from clients and the case management professional community about who can provide these services.
SDoH Assessment: G0136
Unlike the social drivers of health screening in the inpatient setting, this SDoH assessment is a 5-15 minute add-on assessment to an existing evaluation and management (E&M) visit or annual wellness visit with a provider to assess social factors that may be impacting a patient’s health status. The assessment must include the domains of housing, food, utility, and transportation needs or insecurity. Consideration should be given to utilizing the Centers for Medicare & Medicaid Services’ (CMS’s) cited SDoH screening tools for convenience to help facilitate conversation, but it is not required. These approved tools can be completed as a self-exam by the patient in the visit; however, the responses and applicable needs must be pulled into the provider’s documentation. CMS has made it clear that in order to bill for G0136, the provider cannot simply screen for SDoH, but must demonstrate an assessment of need and its impact in the medical visit.
For instance, the patient may complete their Health-Related Social Needs (HRSN) Screening Tool in the lobby prior to the visit, through which they identify that they are struggling with keeping food on the table in their house. During their annual wellness visit (AWV) with their provider, they then discuss how food insecurity has impacted their ability to manage their diabetes. This finding is then incorporated into their care plan, and the patient is referred to the clinic’s case management program to assess further needs to support diabetes management and layout community food options. Ideally, there would also be Z codes that are captured as a result of the documented SDoH factors assessed.
Say the HRSN tool was provided to the patient, yet no SDoH needs were identified – then the provider would have no need to incorporate or bill for G0136 during their visit. The patient would screen negative and be listed as having no further needs. This code can billed every six months, which would allow the provider to follow up with their patients regularly should social factors change, requiring adjustments to the medical plan of care because of new considerations related to social domains.
Community Health Integration: G0019 and G0022
The Community Health Integration (CHI) codes are billed as a monthly charge, initiated after a provider visit in which community health integration needs are identified related to specific SDoH concerns that are impacting the patient’s medical treatment. G0019 is for 60 minutes in the month in which services are performed “incident to” by a community health worker or trained auxiliary personnel representative who is able to assist the patient in addressing their SDoH needs, such as obtaining food assistance, completing a housing voucher, or obtaining a monthly bus pass.
Community health workers (CHW) are typically frontline public health workers who are trusted members of the local communities they serve. They serve a unique role in receiving training and/or certification to link the healthcare system to local social services and the cultural community. These individuals may provide translation services and typically reside within the community in which they are working. These individuals may work directly under a provider, or serve as auxiliary staff connected under the social work and/or case manager to provide “on-the-ground” and in-home support services for patients receiving services through nontraditional means.
For G0019 to be utilized, there would need to be an initial assessment that would determine the appropriate services and goals that are going to be accomplished between the CHW and the patient. There would then need to be continued documentation demonstrating progress and contact between the patient and CHW throughout the month that demonstrates the time expectation. G0022 would be added for each additional 30 minutes beyond G0019 that is completed within the month.
Ideally, there would also be Z codes that are captured based on the findings from the provider’s initial visit and the CHW assessment and treatment goals.
Principal Illness Navigation: G0023, G0024, G0140, and G0146
Principal illness navigation (PIN) can best be understood as providing reimbursement to navigators who work with patients with significant chronic conditions. To qualify for PIN, these conditions, such as cancer, chronic obstructive pulmonary disease (COPD), congestive health failure, or HIV/AIDs, must exist for greater than a three-month duration and must present with enough significance that there is risk of hospitalization, nursing home placement, decompensation, or decline, should the condition not be addressed or treated. PIN is billed as incident to where the provider, through an initiating visit, identifies that the patient would receive PIN services appropriately to support and navigate the complexity of their condition(s) to guarantee access to services and avoid unnecessary decline.
G0023 serves as a monthly charge: 60 minutes of time initiated via verbal or written consent for a trained and/or certified professional to provide and assess a patient under the supervision of the provider. This individual would complete a biopsychosocial assessment and treatment plan that would connect the member’s condition to potential SDoH risk factors and identify need for education or supportive navigation services to coordinate care. G0024 would be billed for an additional 30 minutes of services in the month. All information and connections with the patient would be documented with capture of time and updates on treatment and goal progress. At this time, the specialist is listed generically for PIN services; however, in most clinical settings, a chronic disease navigator is often a nurse or social worker. These codes would allow for those individuals to count their time in working with patients to address their disease, medication needs, and psychosocial needs through the treatment planning and intervention process for reimbursement under the patient’s attending provider.
G0140 and G0146 are similar codes; however, they correspond to the principal diagnosis for navigation services in the behavioral health setting. These codes include circumstances in which the “incident-to” specialist is a certified peer support specialist, which is a specific call-out and varies from the PIN chronic medical disease codes. The SDoH, CHI, and PIN codes are a step in the right direction towards acknowledging the social factors that impact patient complexity of care and navigation of the medical landscape. There are some unknowns in the specialization of certified professional skill sets in each of these codes, which are still broadly defined. Additionally, it appears that these codes are allowed to be billed in conjunction with chronic care management and remote patient monitoring as long as the time is not duplicative, and services are appropriately documented as medically necessary and socially relevant for the patient.

Livanta Offers Cerebral Edema Recommendations
A condition may be diagnosable, but not relevant if it does not impact the current encounter. A diagnosis is not codable if it is not documented in an appropriate format.
By Erica E. Remer, MD, CCDS
Dr. Ronald Hirsch inspired this article – months ago, he asked me to look at a publication from Livanta and comment on it.
Livanta is a Beneficiary and Family-Centered Care Quality Improvement Organization (BFCC-QIO), and one of its jobs is medical case review, to ensure that Medicare patients in their jurisdiction are receiving medically appropriate care and services. Their monthly publication, The Livanta Claims Review, from last August focused on the condition of cerebral edema (The Livanta Claims Review Advisor, Volume 1, Issue 19).
In it, they quote the Recovery Audit Contractor (RAC) Statement of Work in that “clinical validation involves a clinical review of the case to see whether or not the patient truly possesses the conditions that were documented in the medical record.” Livanta asserts that “clinical validity reviews are performed by currently practicing physician reviewers. The most common reason for denial of cerebral edema on claims is a failure of the provider to document the clinical information that supports the diagnosis – there is often no documentation of cerebral edema at all until the post-discharge query. It is vital for providers to document the clinical information that led to the diagnosis of cerebral edema rather than simply stating on a query that it is present.”
We must keep in mind that reviewers are making their judgments solely based on the available documentation.
It is completely legitimate to expect documentation to demonstrate that a condition being claimed and coded is clinically valid. The Livanta publication also has a section on Good Documentation Practices. Their expectation is that there will be documentation of the following:
Clinical signs or symptoms such as headache, vomiting, altered mental status, or seizures;
Findings on imaging. They only mention MRI, but CT scans may also reflect changes consistent with cerebral edema. They offer phraseology such as “brain compression,” “displacement,” or “midline shift.” I will add “mass effect” to their list. Later on in the document, they note that “vasogenic edema” isn’t found in the coding index, specifying that the words “cerebral” or “brain” must be linked with “edema;” and
Clinical significance supported by documentation of treatment. Corticosteroids, mannitol, surgical decompression, a plan to monitor with repeat imaging, or a documented linkage between the condition (cerebral edema) and clinical deterioration could serve as evidence that the condition is not just an incidental and inconsequential radiological finding.
Post-discharge queries that result in a diagnosis of cerebral edema after the fact, without evidence of clinical significance, are to be dismissed, according to Livanta’s instructions.
This condition is illustrative of the concept that clinical validity is often predicated on clinical significance. A condition may be diagnosable, but not relevant if it does not impact the current encounter. A diagnosis is not codable if it is not documented in an appropriate format.
Some of you may have seen my macro for sepsis before: sepsis due to (infection) with acute sepsis-related organ dysfunction as evidenced by (specify organ dysfunction/s). This guides the provider to give the etiology and the evidence of clinical significance.
For all conditions, providers should be instructed to document their clinical support (signs and symptoms), any laboratory or imaging evidence bolstering the diagnosis, and what is being done about it (or when treatment is considered, but declined by the patient).
A single reference to a condition is only weak evidence; it is preferable for the discussion and diagnosis to appear multiple times in the record. It needn’t be redundant copying and pasting. Each day the provider should ponder and document how the situation is progressing. Are the symptoms improved? Are there new or worsening clinical indicators? Is the treatment succeeding, or does it need adjustment? A single mention in a post-discharge query very well may not be adequate support of a codable diagnosis, because if it was clinically significant, wouldn’t it have been noted and treated prior to discharge?
For this targeted condition, consider this model documentation:
Cerebral edema due to known glioblastoma, as evidenced by severe headache and projectile vomiting, new since Friday. MRI confirms increased brain compression and cerebral edema. Will administer dexamethasone and consult neurosurgery to assess for urgent decompression.
Determination of clinical significance shouldn’t be left to the imagination or whim of the reviewer. The provider should think in ink and explain why they are making their diagnoses (and what they are doing about them). Clinical documentation improvement specialists (CDISs) should do their traditional querying early to get the diagnosis input promptly. If there is inadequate support in the documentation, a clinical validation query may be indicated to ensure that the diagnosis is removed if not valid (or documentation is improved if it is valid).
Training the provider to supply linkage and evidence of clinical significance is a good proactive step. And it is a best practice for the diagnosis to appear when first noted, as it is treated, and as it resolves, and then brought back into the spotlight in the discharge summary.

Does Coding Clinic Allow Payers to Make Their Own Clinical Criteria?
It has been brought to my attention that some payers are citing the American Hospital Association (AHA) Coding Clinic, pages 147-149 of the 2016 fourth-quarter edition, to justify using their own criteria as the basis for denials.
By Erica E. Remer, MD, CCDS
I would like to focus on clinical criteria today. It has been brought to my attention that some payers are citing the American Hospital Association (AHA) Coding Clinic, pages 147-149 of the 2016 fourth-quarter edition, to justify using their own criteria as the basis for denials.
The Coding Clinic advice attempts to explain Guideline I.A.19, “the assignment of a diagnosis code is based on the provider’s diagnostic statement that the condition exists. The provider’s statement that the patient has a particular condition is sufficient. Code assignment is not based on clinical criteria used by the provider to establish the diagnosis.”
It is ironic that this guideline is specifically intended to explain that the coder is not permitted to assume diagnoses according to any published criteria, and then payers want to use this advice to justify their being able to discount diagnoses according to their own criteria.
The provider “may use a particular clinical definition or set of clinical criteria to establish a diagnosis,” but Coding Clinic cautions that the code is purely based on the documentation. The guidance states that “a facility or a payer may require that a physician use a particular clinical definition or set of criteria when establishing a diagnosis, but that is a clinical issue outside the coding system.”
I don’t think they mean the word “may” as in “we are granting them permission.” I think they mean the word “may” in the sense of “might.”
Let’s dispel this fallacy right here and now. I have yet to see a facility that strictly mandates a physician to use a particular clinical definition or set of criteria to make a diagnosis. The organization may convene an internal group to discuss a condition and what they would like to see in order to make a diagnosis, but there is always some disclaimer in the written policy that the provider must be permitted to use their clinical judgment. I recommend that they call their internally derived recommendations “internal clinical guidelines.” A guideline is a statement or declaration of policy that sets general standards for an agency or facility but does not have the force or effect of law.
If a provider is not following an internal clinical guideline for a considered reason, they should document the rationale for their deviation. If there is concern that the provider has acted way out of the boundaries of generally accepted medical care, then there should be a clinical quality review of the care. The provider’s medical colleagues are qualified to judge whether they believe care was appropriate after an investigation, in the context of a specific patient and that provider’s past actions.
If payers are using generally accepted consensus-based criteria to judge medical care, then it is reasonable to generate clinical validation denials if the provider has substantially deviated. For instance, a provider made a diagnosis of acute kidney injury (AKI) with a creatinine of 1.6, but the patient had a baseline of 1.4 with known chronic kidney disease (CKD), stage 3a. Generally accepted KDIGO (Kidney Disease Improving Global Outcomes) criteria for AKI are an increase of serum creatinine of greater than 0.3 mg/dL within 48 hours or more than 1.5 times the baseline within the prior seven days. Unless the practitioner has some compelling underlying reason for departing from the criteria that they hadn’t documented, it would be understandable to deny the assertion of AKI in this patient.
But a payer should not be able to demand that for the diagnosis of AKI; the creatinine elevation must be greater than 2.0 mg/dL within 24 hours, just on their whim, apparently. It is unreasonable for payers to create their own proprietary clinical criteria that have no discernible basis in science or medicine, and for insurers to be allowed to require facilities to adhere to those secret criteria.
The Coding Clinic segment recognizes that clinical guidelines may be crafted by institutions or payers, but affirms that coding experts do not have the authority to validate criteria; as they note, it is out of the scope of the coding system.
If you have contracted with a payer and there is a stipulation that they may use their own clinical criteria to determine clinical validity, you should either insist that you have access to their established criteria, or better yet, strike that from the contract.
Making diagnoses and documenting them is not for the sake of the payer. It is for the patient. The provider is trying to deliver optimal care and report it accurately. If a payer quotes this Coding Clinic advice, include in your appeal:
The Coding Clinic advice states, “Only the physician, or other qualified healthcare professional legally accountable for establishing the patient’s diagnosis, can ‘diagnose’ the patient.” Furthermore, although Coding Clinic is giving its recommendations, they are also acknowledging that it is not up to them to rule on whether a particular definition or set of criteria are valid to establish a diagnosis. They explicitly state that it is out of the realm of the coding professional.
My advice is for facilities to have ongoing discussions about changing and current clinical criteria to foster best clinical practice. Providers should be instructed to document their thought process well and in a codable format. Clinical validation queries should be composed to ward off clinical validation denials, as per the last sentence of I.A.19.: “If there is conflicting medical record documentation, query the provider.”
If a payer denies a claim due to legitimate clinical validation concerns, give the money back; it was a loan. If they are making up capricious criteria to unjustly deny proper diagnoses, don’t take that lying down.
If they quote this Coding Clinic advice as being support for their being allowed to make up their own criteria and hold you to them, fight it.
And make sure the folks who enter into contract negotiations don’t sanction it, either.
Listen to Dr. Remer today when she cohosts Talk Ten Tuesdays with Chuck Buck at 10 Eastern.

Take the Time to Get Time-Based Billing Right
Since Jan. 1, 2023, practically speaking, all evaluation and management (E&M) service coding is based on medical decision-making or time. And some providers are not documenting time appropriately.
By Erica E. Remer, MD, CCDS
I am currently performing a fraud assessment, and since I can’t go back and educate the provider in question, I am going to share my insights with you. Since Jan. 1, 2023, practically speaking, all evaluation and management (E&M) service coding is based on medical decision-making or time. And some providers are not documenting time appropriately.
It’s no longer only face-to-face (F2F) time or time spent on the floor or unit that counts. It is the total time devoted to the patient, which includes some component of F2F time on the day of the encounter.
Consider the following:
The face-to-face time may be delivered by another qualified healthcare professional, as opposed to the ultimately responsible billing individual, if the time is split/shared or incident-to.
Counseling and coordination of care not separately billed for may be counted, but there is no longer a threshold of greater than 50 percent of the time. That should be removed from any attestations.
Time need not be continuous, but you can only count time solely devoted to the patient for that given time interval. Maybe it is your practice to review labs in the morning before you start your rounds or your office hours. Then, a few hours later, you see the patient and do a history and physical. You order some tests (the time clicking in the electronic medical record counts), which you discuss afterwards with the patient because it informs your shared decision-making. You prepare discharge instructions. At the end of the day, you spend quality time with the electronic health record (EHR) documenting the encounter. All of that time can be added up and claimed. Remember:
It may not be practical to use a time-tracking app, but you should be able to guesstimate accurately. Be truthful. Time spent on separately billed activities should be carved out. You can’t double-dip.
If two individuals see the same patient at the same time, providing the same service (e.g., rounding together), only one of them can claim any given moment in time. You can’t double-dip.
Don’t give a range of time, e.g., 30-74 minutes. Some time-based services, like critical care, can be additive. What number would you use to add? How can you tell if prolonged services add-on is appropriate if a range is given?
Don’t document “approximately 35 minutes.” Does that mean “34 minutes,” which is under the threshold, or “36 minutes,” which crosses it?
Similarly, don’t document “greater than 35 minutes.”
Detail some activities you are including in your time-based billing. If you have a standard macro, I strongly recommend editing it to reflect the services you provided today, with this patient.
Personal chit-chat, although it can take time, cannot be counted in time-based billing. There are specific activities that are permissible (see https://www.ama-assn.org/system/files/2023-e-m-descriptors-guidelines.pdf) to be counted.
Remember that an auditor is looking at documentation over time and over multiple patients. If you only use macros or templates or copying and pasting the reviewer will notice. The auditor will be trying to get a feel of what you are doing over the course of the day. Did you really perform that physical exam if it is identical from patient to patient, and never changes over time?
If your documentation has a field to put the date and time seen, try to be accurate. Unless you are office-based and never run late or have issues that throw your schedule off, it looks suspicious to run exactly on the hour or half-hour for every patient, every day. In the hospital? You never used the restroom or grabbed a snack or answered a phone call or got waylaid in the hall by a nurse?
If you have fields where you put start and stop times for your F2F time, label them as such. As noted, there are a lot of other activities that may be counted in time-based billing, and it is perfectly reasonable that you wouldn’t be documenting to account for those administrative and not-in-the-presence-of-the-patient times in the progress or office note. But it looks funny if it says at the top of the note, “Time: 4:00-4:30 p.m.” and at the bottom of the note, it just says “35 minutes were spent.” This is an internal inconsistency.
It looks suspicious if you run back-to-back 30-minute intervals all day long, claiming 35 minutes for each, and completing the documentation before you see the next patient. It looks really bad if you document that you saw a patient when the nurse records they were sleeping. It is impossible to see patients in the drive time between facilities. You can’t prospectively document an encounter.
In this day and age, assume that investigators will be able to ascertain where you physically were. Don’t lie and say you were at the hospital when you were in the grocery store or in another state.
Remember that electronic records have an audit trail. You may (truthfully) assert that you saw a patient at 10 a.m. while documenting the encounter at 1 p.m., but you can’t fix it, so the computer says you typed it at 10 a.m.
In order for an encounter to be billable, it needs to meet medical necessity. If the medical decision-making is moderate, but the patient requires more time than is typical for a 99232 (subsequent hospital care) because they have a lot of questions, a 99233 can be justified on the basis of time. However, if a patient is completely stable and has no new problem, and there no studies to analyze or changes in medication or plan of care, and they are to be discharged the next day (i.e., = 99231), you are hard-pressed to claim the highest level of service. Why did it take you so much time?
Here are my recommendations:
Only put your billing-by-time attestation on the encounters for which you are billing by time. It is confusing for your selected level of service to be one level, but the time attestation would support a different level. It calls into question the veracity of the time attestation on all patients.
Be consistent. If you have start/stop times documented, but are claiming the encounter took more time, explain the discrepancy – e.g., “38 minutes spent, which includes 20 minutes face-to-face, as noted above, review of labs, ordering tests and neuro consult, and documenting in EHR.”
Don’t let your times add up to more hours than it is humanly possible to work in a day.
Tell the truth. Do good-faith guesstimates. Don’t always use the same number. Feel free to not use round numbers, like using 31 as opposed to 30.
You won’t get in trouble for the occasional 35-minute encounter being claimed as 38 minutes. You will get in trouble if you claim one hour when you only spent 17 minutes.
Take the time to get time-based billing right. If you provided the service, you want to be appropriately compensated.

Compliant texting of patient orders approved by CMS
On February 8, CMS released a memorandum outlining new guidelines and permission to text patient information and patient orders to health care team members.
Christmas has come very early this year from CMS to our case management teams! On February 8, CMS released a memorandum outlining new guidelines and permission to text patient information and patient orders to health care team members. Of course, it will be required to take place through a HIPAA-compliant secure texting platform and in compliance with the Conditions of Participation (CoPs). We recommend you meet with your compliance and IT teams to discuss the next steps to texting status change orders. This new ruling is effective immediately and applies to both acute hospitals and critical access hospitals.
The link below will take you to the link to view the CMS memorandum related to this new change:
https://www.cms.gov/files/document/qso-24-05-hospital-cah.pdf

Federal Officials Seeking to Mitigate Maternity Deserts
The Centers for Medicare & Medicaid Services (CMS) just released news that they will be working on a 10-year payment and care delivery model called the Transforming Maternal Health Model (TMaH).
By Tiffany Ferguson, LMSW, CMAC, ACM
If you came across my recent blog article on the significant concern of “maternity deserts” in the U.S., as you will recall, the widely accepted definition of the phenomenon is any county lacking maternity care units.
The Centers for Medicare & Medicaid Services (CMS) just released news that they will be working on a 10-year payment and care delivery model called the Transforming Maternal Health Model (TMaH). This model strives to support participating state Medicaid agencies in developing and implementing a whole-person approach to pregnancy, childbirth, and postpartum care for women with Medicaid and Children’s Health Insurance Program (CHIP) coverage.
There are not a lot of details yet on how this program is going to be fleshed out, other than generic reference to key terms such as data, research, and evidence-based practice. However, I anticipate that more information will be coming in the first quarter of this year.
What we know so far is the following:
This program will be directly tied to the CMS “Birthing- Friendly” designation.
This program will be offering participating state Medicaid programs $17 million over a 10-year period.
Participation will encourage increased coverage and funding for maternal health providers such as midwives, doulas, and freestanding birthing centers.
The approach will emphasize a whole-health strategy from pregnancy to post-partum, with care delivered to both mother and child for social and medical needs.
The approach is looking to technology to fill in gaps, such as remote patient monitoring for high-risk obstetrics coverage.
CMS is planning to release a notice of funding in the spring of 2024, with application submission requirements later in the year. Only 15 states will be awarded acceptance, with kickoff in January 2025.
Although I am thankful for the financial opportunity, and I don’t want to appear ungrateful, I am concerned about how this will end up trickling down to create scalable impact. Completing some quick math, $17 million divided per year would be $1.7 million annually for an entire state.
Let’s assume the Medicaid plan takes 20 percent prior to this going to the provider level, leaving $1.36 million to split – and this is just a conservative estimate. I am also concerned about what the other 35 states are going to do without the additional funding, as well as what health systems should consider for this year since funding would not begin until 2025. To learn more, click here: Transforming Maternal Health (TMaH) Model | CMS

The Impact of Poverty on Health-Related Outcomes: Data Released
I think this report confirms some of the information we have already seen in our hospitals and EDs: that our patients are increasingly more socially and medically complex.
By Tiffany Ferguson, LMSW, CMAC, ACM
The U.S. Office of Minority Health (OMH) released last Tuesday new public files on Socio-demographic and Health Characteristics of Medicare Beneficiaries Living in the Community by Dual Eligible Status in 2021. The data file provides aggregated demographic information with correlations to health status and chronic conditions, activities of daily living, mental health, and oral health data from Medicare-Medicaid beneficiaries.
This report is a sign of continued federal efforts to release valuable information regarding the social factors impacting healthcare for the Medicare population, which can help inform future policy and practice decisions. The data set from 2021 reveals some interesting details about the uniqueness of the dual-enrolled Medicare-Medicaid beneficiaries and their care delivery needs, compared to those who are not dual-eligible.
Overall, we learned that 26 percent of dual-enrolled members speak another language than English at home, compared to only 9 percent of the population that is Medicare-only. We also learned that over 40 percent of this population was classified as having fair or poor health, compared to only 18 percent of the Medicare-only group. When it comes to activities of daily living, those who were dually enrolled had greater difficulty with walking, bathing, getting out of bed, and dressing themselves than their counterparts, suggesting a greater need for additional supportive services. This also suggests further concerns regarding the progressive nature of poverty and one’s health status.
In looking at how Medicare beneficiaries were functioning in social domains, the impact of poverty was overwhelming in showing a significant decline in access to basic resources for those below the poverty line. A total of 42 percent of those who are 0-138 percent of the federal poverty level do not drive or have given up driving altogether.
This subgroup was also more likely to decrease meal size or skip meals altogether due to lack of access to food, reported at 40 percent. This group was more likely to have trouble staying up-to-date with their preventative healthcare and annual age-related vaccines, such as pneumonia, shingles, and flu. In looking at the neighborhood domain, this population was more likely to either be living alone or in an “other” type setting, likely a placement facility.
They were also significantly more likely to reside in a “disadvantaged” neighborhood, according to the Wisconsin Atlas neighborhood indicator. Not only does this population struggle with social domains, but they are also more likely to have four or more chronic conditions.
I think this report confirms some of the information we have already seen in our hospitals and EDs: that our patients are increasingly more socially and medically complex. Although details were listed in the report regarding patient data, at this time there were not further suggestions for care delivery models; however, I think we have already seen the release of additional funding support for care navigation and provider time to care for this population.
I would imagine that we will continue to see additional resources as we prepare to support the growing number of seniors in our Medicare population who will fall into the dual-enrolled group, as the data confirms their needs are significantly more complex and resource-limited.
Artificial Intelligence Documentation Prompts Must be Compliant, Too
Queries, whether placed by a CDI specialist or an AI solution, need to be compliant and cannot lead providers.
By Erica E. Remer, MD, CCDS
Today I would like to share my opinion on proactive provider documentation decision-making technology. I am completely supportive of genuinely concurrent (that is, occurring in real time) clinical documentation integrity (CDI) efforts. However, I am afraid that the desire to leverage artificial intelligence (AI) can tend to push compliance to the wayside.
Think of the kind of dialogue that occurs when CDI specialists (CDISs) round with providers. Their goal is to generate verbal queries on the fly. When done compliantly, the CDIS shouldn’t lead the provider to alter their documentation; they should give them the necessary facts and clinical indicators, which permit the clinician to make a good, informed decision about best-practice documentation.
Why can’t we use technology to perform the same role? I think we can, but the programming that goes into the algorithm and offered choices needs to be done with care and in a compliant fashion.
I have spoken with representatives from multiple companies who are developing this type of technology, and they all resist the notion that these proactive, real-time documentation alerts are “queries.” The organizations that establish our CDI standards – the Association of Clinical Documentation Integrity Specialists (ACDIS) and the American Health Information Management Association (AHIMA) – are pretty clear that they do consider these queries.
In the ACDIS/AHIMA position paper on Guidelines for Achieving a Compliant Query Practice (2022 Update), they say, “the purpose and expectations of the documentation query process are to assist the provider in creating thorough and complete documentation, including specificity, treatment provided, and clinical validation. All queries must meet the same compliant standards, regardless of how or when they are generated, including those autogenerated by artificial intelligence (AI) and computer-assisted coding (CAC), whether in real-time computer-assisted physician documentation (CAPD) or after the episode of care is complete.”
There is also another ACDIS/AHIMA publication called Compliant Clinical Documentation Integrity Technology Standards, which asserts that any technology used to identify documentation opportunities must follow the guidance in the Guidelines for Achieving a Compliant Query Practice.
Some refer to these documentation alerts as “nudges.” This is defined by Merriam-Webster as “a slight push, poke, or jog (as with the elbow).” The word “leading” is defined in the dictionary as “guiding, directing.” Just by using the word “nudge,” it evokes the prohibited action of leading, because isn’t the point of a nudge to push the recipient in a predetermined direction?
Some real-time notifications are indisputably compliant. If a doctor has documented “heart failure,” instructing them to provide clarification as to specificity and type without providing specific choices is totally reasonable. The clinician has already established the diagnosis; the electronic CDI tool is merely asking for further detail.
If the computer is selecting clinical indicators and offering clickable potential diagnoses, it can get more complex. It needs to offer all diagnoses that can meet the applicable clinical indicators, and I would suggest that there should be a mechanism for the provider to reject all of them and/or explain their thought process. The ACDIS/AHIMA position paper on compliant querying states that “if a query response from a technology-driven query does not yield the response desired, it is inappropriate to send a follow-up manual query, for the same diagnosis/condition/procedure, in absence of new clinical indicators.”
If the provider just ignores the alert or isn’t given a choice of “I choose none of those offered,” how would the CDIS know that they shouldn’t manually query once they find the opportunity on their own review? The technology standards paper states that “all queries should be memorialized to demonstrate compliance with all query requirements and validate the necessity of the query.” Where are these documentation prompts with their instantaneous turnaround times memorialized?
I once saw a demonstration of one of these technologies, and the provider was offered the clinical indicators of an ejection fraction of 25 percent, with the patient having been administered a dose of diuretic, and the only choice offered was acute systolic heart failure. I pointed out that this could also be consistent with acute-on-chronic systolic heart failure, acute systolic and diastolic heart failure, and acute-on-chronic systolic and diastolic heart failure. Being given a single choice was misleading – or should I say, leading?
What if the technology noted an abnormal lab finding, such as a sodium of 131, and presented it as “an electrolyte disorder is noted. Please specify type.”? Again, this is not compliant. The provider has not already established that there is “an electrolyte disorder;” the e-CDIS is drawing a conclusion and making a diagnosis for them. It would be acceptable if the alert read, “there is an abnormal electrolyte level. Is there a corresponding diagnosis?” If asked my advice, I would actually recommend something like, “is there a clinically significant corresponding diagnosis?” and there would either be a reminder or provider training to document how the condition was being assessed, treated, or monitored. Without demonstrating clinical significance, it is not a codable diagnosis.
The Compliant CDI Technology Standards cites how computer-assisted provider documentation using AI and delivering prompts differs from information available for educational purposes on general CDI topics. The essential difference is that the prompt is case-based, and focused on details unique to each patient. This renders it a query.
There is guidance as to how to select a compliant CDI vendor in the Technology Standards paper. My advice is start with: “these are queries, and, as such, they need to be compliant.” Then, run with it. Everyone else is!

Lessons to Learn from OIG HCC Reviews
If your facility has not taken steps to ensure that Hierarchical Condition Category (HCC) diagnoses are properly validated, you are just asking to be the next victim in the OIG headlights.
By Erica E. Remer, MD, CCDS
The U.S. Department of Health and Human Services (HHS) Office of Inspector General (OIG) released a report on a Medicare Advantage Compliance Audit of SelectCare of Texas, Inc. The findings of the report — published at the end of November (2023) — were reminiscent of those of the OIG’s review of Geisinger Health Plan in the spring, and Excellus Health Plan in the summer. This audit reinforces the lessons that should be learned.
There were a set of nine conditions appearing in this audit, which were identified by data-mining and discussions with medical professionals. It seems to me that the issue was roughly the same for each category – a diagnosis was claimed and there was no evidence of treatment or continuity. It also seems as though this set of diagnoses was identical to that found in previous audits.
Acute stroke – there must be a corresponding inpatient or outpatient hospital claim within the service year. Patients do not have chronic strokes, although they may experience sequelae from a previous stroke. The coding can distinguish between a current, acute cerebrovascular (CVA) accident and a previous CVA with residua. As I have said before, if an outpatient provider has the urge to document and code an acute stroke, they should be calling 911 for transport.
Acute myocardial infarction (MI) – if an acute MI code isn’t found on an inpatient claim within 60 days, then the OIG questioned whether a less-serious condition wouldn’t be more appropriate, like angina pectoris, myocardial injury, or some other ischemic heart disease. Acute MI is picked up for 28 days after the initial diagnosis, but their presumption is that there would have been an index admission.
Major depressive disorder – if the condition were captured on only a single claim during the service year, but no antidepressant medication was dispensed, the OIG felt the diagnosis might be considered unsupported. I wondered:
What if the patient opted for psychotherapy instead of medication?
What if it were discovered at the end of the service year? It might still be clinically valid if the documentation supported it.
Embolism – suspicion arose if there was only one claim with this diagnosis in the service year and no anticoagulant medication had been ordered. Musings:
What if the patient has or had an inferior vena cava filter placed? This is usually because there is a contraindication to initiating anticoagulation.
This is a diagnosis that has codes available for acute (including subacute), chronic, and history of. Providers need to select the clinically valid code.
Vascular claudication – these enrollees had the diagnosis found on only one claim, but had not had one of the diagnoses that indicate vascular claudication during the preceding two years – and, furthermore, they were taking a medication usually associated with neurogenic claudication.
Lung, breast, colon, and prostate cancers – if there was an active cancer diagnosis on only one claim, but there was no surgery, radiation, or chemotherapy administered within six months prior to or subsequent to the diagnosis, the OIG concluded that a “history of” cancer code should have been used instead.
Immunotherapy is a commonly utilized treatment for certain cancers now. It does not seem to be on the OIG’s radar.
What if a patient declined treatment? The condition is still valid.
Diagnoses that are chronic should be coded as chronic. Having a single documentation of a chronic condition calls into question whether it is really present. Having a chronic condition with a standard-of-care medical treatment should result in that treatment being prescribed unless there are contraindications or extenuating circumstances (which should then be laid out in the record).
One of the cancers was denied because only “lung mass” was documented. This reinforces the position that it is advisable to document pathology diagnoses post-discharge. There was also a lung metastasis, which was submitted as a primary malignancy. The most common issue regarding cancers was that they should have transitioned to “history of,” but had instead been submitted as active, current conditions.
There are multiple prongs to the approach to solving this problem. The first is educating your providers on correct documentation and coding. They need to document conditions accurately and precisely. They need to choose the correct code, supported by the documentation. When diagnoses evolve to “history of,” the documentation should follow suit.
When a diagnosis is made, medically appropriate treatment should be initiated unless there are extenuating circumstances preventing that course of action. That should be explicitly recorded in the chart.
Your organization should consider setting up a technology solution to ensure that any of the high-risk target conditions have evidence of treatment or an explanation as to why treatment is not being undertaken. Perhaps an electronic medical record alert for a programmed set of diagnoses? A reconciliation of diagnoses and administration of medication? A second-level review by clinical documentation integrity (CDI) for high-risk diagnoses?
It should be routine practice that when a chronic diagnosis is made, it is documented repeatedly during a service year whenever it is being addressed. In theory, noting a diagnosis once is sufficient for coding; in practice, auditors question chronic diagnoses if they are only mentioned once and never again.
If your facility has not taken steps to ensure that Hierarchical Condition Category (HCC) diagnoses are properly validated, you are just asking to be the next victim in the OIG headlights.
An ounce of prevention is worth a pound of recoupment.
Programming note: Listen to Dr. Erica Remer as she co-hosts Talk Ten Tuesdays with Chuck Buck today at 10 Eastern.

News Highlights for SDoH to Start off 2024!
As we step into the new year, the mix of social needs and healthcare will continue to demand our attention.
By Tiffany Ferguson, LMSW, CMAC, ACM
Happy 2024! This article will focus on a couple of news highlights that emerged over the holiday break.
First, the LOINC and Health Data Standards by the Regenstrief Foundation, developed in partnership with the Gravity Project, have been awarded a $4 million grant to support an initiative to standardize documentation and data elements in electronic medical records (EMRs) for social determinants of health (SDoH) collection.
Currently, SDoH elements in patient medical records range from free text notes to specific data fields. These fields are in variable locations of the medical record and are often customized not only by the type of EMR but also by hospital location, making it nearly impossible to develop scaling information. This project aims to improve current conditions and to standardize SDoH data elements such as food access and neighborhood safety.
Second, maybe some of you will recall the Medicaid unwinding last year when state Medicaid plans had to fall back into compliance with the removal of federal protections from the COVID-19 pandemic. This has been a struggle, understandably so, with the gap in years and providers now trying to track down reenrolling information or qualify adults and children who are Medicaid-eligible. Over the holiday break, the Centers for Medicare & Medicaid Services (CMS) made public acknowledgments commending states that followed automatic renewal practices and condemning the 10 states that elected not to expand Medicaid coverage, leading to increased disenrollment. Those 10 states have a combined rate of disenrolling children more than the rest of the country’s enrollment rate. The highest category of disenrollment was 19-year-olds, who accounted for 27.6 percent of the total across the non-Medicaid expansion states.
Federally, CMS is concerned, because there is a coverage decline of approximately 35 million children between pre-pandemic and 2023 Medicaid Children’s Health Insurance Program (CHIP). U.S. Department of Health and Human Services (HHS) Secretary Becerra did issue letters, which are publicly available, to the nine states with the highest disenrollment rates by numbers and percentage. Becerra also provided recommendations to combat their declining rates and encourage enrollment and healthcare coverage, such as decreasing call times and eliminating burdensome processes for reenrollment. The letters also called again for applicable states to expand Medicaid coverage and remove barriers such as CHIP enrollment fees or premiums.
As we step into the new year, the mix of social needs and healthcare will continue to demand our attention. The initiative to standardize SDoH data collection marks a positive stride toward greater data and documentation alignment.
Meanwhile, challenges persist with Medicaid, demonstrating the continued need for proactive measures to address disenrollment and ensure healthcare access, particularly for children and young adults.
These events emphasize the ongoing importance of unified efforts to navigate healthcare complexities and promote equitable access to services.
Programming note:
Listen to Tiffany Ferguson report this story live today during Talk Ten Tuesdays with Chuck Buck and Dr. Erica Remer, 10 Eastern.

Maternity Deserts: The Growing Concern of America’s Maternal Care
Today is it is estimated that more than 2 million women of childbearing age live in maternity care deserts, meaning they reside in counties that do not have obstetric care, many of them rural.
By Tiffany Ferguson, LMSW, CMAC, ACM
It has been about six months since I last reported on the growing concern of maternal care, and in particular, the known issues of maternal mortality rates among African-American women.
A couple of weeks ago, Timothy Powell reported on the Centers for Medicare & Medicaid Services (CMS) “birthing-friendly” designation icon. However, is an icon really enough? The responsibility still seems to lie heavily on the provider’s side, and I am concerned that we have not seen the depths of our maternal health crisis just yet.
In late 2023, yet another maternity ward, this time in Monroe, Alabama, closed its doors after many last-ditch efforts to preserve a much-needed but severely underfunded resource. In Monroe, where the population grapples with a 22-percent poverty rate, residents now face the expectation of traveling beyond county lines to neighboring hospitals for labor and delivery services. The travel is expected to be anywhere from 35 to 103 miles, each way. This closure marks the third maternity unit that has closed its doors this year in Alabama because of financial constraints and limited availability of willing providers to practice in the state, because of its strict anti-abortion guidelines. Physicians are not willing to take the risk and the hospitals cannot survive otherwise, to provide the much-needed care for their communities.
In October 2022, the U.S. Government Accountability Office (GAO) released a report on maternal health, urging for governmental support and intervention in the growing decline of obstetric services in rural areas since 2014; over half of all U.S. counties no longer had hospitals with labor and delivery services, as of 2018.
Today is it is estimated that more than 2 million women of childbearing age live in maternity care deserts, meaning they reside in counties that do not have obstetric care, many of them rural. In 2022, it was reported that 13 labor and delivery units closed, and unfortunately, this number continues to grow. In California alone, 11 maternity wards have closed in 2023, with only one maternity ward opening.
Maternity care deserts have been associated with a lack of adequate prenatal care, limited to no treatment for pregnancy complications, and increased risk of maternal death.
The top reason for the closures is money, as Medicaid funds about 50 percent of all births nationally, and more than half of births in rural areas.
The second reason is a national shift in declining birth rates.
The third stems from the unintended consequences of more stringent abortion laws, which have put many obstetric providers in a difficult position regarding adherence to nationally recognized care guidelines and state mandates when prenatal complications arise.
In review of CMS maternity initiatives, the focus appears to be on provider quality initiatives, rather than funding support. The only alternative efforts to combating maternity deserts appear to be the growing availability of telehealth to support prenatal care needs and the expansion and support for midwifery services.

Rebooting “Observing the Rules for Observation After Outpatient Surgery”
Written in March 2013 by the highly respected Dr. Steven Meyerson, “Observing the Rules for Observation after Outpatient Surgery” evolved over time into one of the most-read articles in the history of RACmonitor.
By Juliet Ugarte Hopkins, MD
Written in March 2013 by the highly respected Dr. Steven Meyerson, “Observing the Rules for Observation after Outpatient Surgery” evolved over time into one of the most-read articles in the history of RACmonitor. This point became extremely relevant to me earlier this year, when my manager of case management rushed into my office, papers in hand, hot off the printer.
“Read this article!” she exclaimed. “I think we might need to change the way we think about patients who are hospitalized after pre-scheduled procedures.”
Reading through the piece (admittedly, for the first time – forgive me, Dr. Meyerson!), it very quickly became apparent that the content should have already been part of my modus operandi, as a physician advisor for my health system. But it was also very clear why my department manager would have no knowledge of this. Which brought the concern to my mind: “What about RACmonitor’s other followers? How will they know what’s happening here?”
Happily, the publisher of RACmonitor, Chuck Buck, along with Dr. Meyerson himself, gave me their blessing to update this classic article, which contained excellent direction and advice before the Centers for Medicare & Medicaid Services (CMS) Two-Midnight Rule came into existence just over 10 years ago. In the following paragraphs, you will see original paragraphs from Dr. Meyerson’s article as well as my remarks.
The rules governing the use of observation for patients undergoing scheduled outpatient procedures are quite different from those that apply to patients coming in from the ED (emergency department) with undiagnosed symptoms or urgent conditions. Placement and billing errors are common, so it is worth reviewing the subject at this time.
This remains true, but the greater point in 2023 is that the finer points of conversion from outpatient to outpatient with observation services for a scheduled postoperative patient require much more deliberate education for physicians, nurses, and case managers. More on that in a bit.
Actually, it’s quite simple: as a rule of thumb, the only time observation can be used for a patient having a scheduled outpatient surgery or procedure is when there is a postoperative complication that prolongs routine recovery. But like most things Medicare, it’s never quite that simple – so read on.
Today, post-Two-Midnight Rule, this is exactly the only time observation can be used for a patient having a scheduled outpatient surgery or procedure – when there is a complication either during the procedure or during the recovery period. While a prolongation of the recovery sometimes comes into play…it’s not a necessity. Anything that requires care above and beyond what was originally expected or anticipated makes a change from outpatient to outpatient with observation services appropriate. This could involve something as simple as nurses performing vitals every two hours instead of every four. The point is that more care or services are being provided to the patient than per the usual routine. Something as subtle as this can sometimes be hard for people to recognize, which is why it is important to be vigilant so observation hours are captured appropriately.
According to the Medicare Claims Processing Manual (Chapter 4, Section 290.2.2), “hospitals should not report as observation care services that are part of another Part B service, such as postoperative monitoring during a standard recovery period (e.g., 4-6 hours).” While this section mentions “4-6 hours” as an example of a standard recovery period, it is important to note that this time frame only is used as an example and does not set an upper limit on the time permissible for recovery. In other words, it would be inappropriate to place a postoperative patient into recovery just because an arbitrary six-hour time period has elapsed. CMS explains that a patient having an outpatient procedure may be expected to stay up to 24 hours: “When patients with known diagnoses enter a hospital for a specific minor surgical procedure or other treatment that is expected to keep them in the hospital for only a few hours (less than 24),” the agency has indicated, “they are considered outpatients for coverage purposes regardless of the hour they came to the hospital, whether they used a bed, and whether they remained in the hospital past midnight.” (Medicare Benefit Policy Manual, Chapter 1.) In this case, “less than 24” does define a time limit on an expected outpatient stay, and this clarifies that a patient’s stay may be overnight in a hospital bed in outpatient status – and still qualify as recovery.
Chapter 4 of the Medicare Claims Processing Manual was last revised on Dec. 22, 2017, but changes were not made to Section 290.2.2. It continues to include the direction mentioned above about not reporting observation services hours in cases of “postoperative monitoring during a standard recovery period (e.g., 4-6 hours).” Again, like before, the timeframe of “4-6 hours” is not a guide on how long recovery should be considered “routine” following a procedure. If one of your surgeons feels “routine recovery” following a procedure involves hospital care for 48 hours, that patient should remain in outpatient status for 48 hours. But you’ll probably want to sit down and figure out why she considers this prolonged time period routine and necessary. Is it truly a best practice and standard of care? Or is it simply the way she’s practiced for the last 25 years?
On the other hand, the Florida fiscal intermediary in 2003 explained that “if the physician intends to keep the patient overnight, especially for 24 hours or more of care at an inpatient level of care (prolonged monitoring given co-morbidity, frequent laboratory studies, frequent IV therapy, etc.), then the physician should schedule an inpatient admission. Also, it is important that physicians document the indications for the procedure and the associated co-morbidities since the medical necessity of the procedure as well as the need for the overnight stay can be reviewed by the QIO (Quality Improvement Organization).” (Florida Medicare A Bulletin, third quarter of 2003.)
This is likely the first paragraph that piqued my manager’s attention, and your first clue that something is awry. Reference to “24 hours or more of care” and “inpatient admission” no longer go together, post-Two-Midnight Rule. Also, with the exception of total knee arthroplasty, as described in the much-obsessed-over 2018 Outpatient Prospective Payment System (OPPS) Final Rule, prolonged monitoring given co-morbidities and/or feared complications that might rear their ugly heads do not support starting with inpatient – or even counting observation hours. For example, a surgeon might elect to keep their patient with a history of asthma who is post-laparoscopic appendectomy in the hospital overnight due to a concern of bronchospasm post-intubation. But observation hours should not be counted unless the patient actually develops respiratory issues that require additional assessment or treatment. If the patient’s recovery overnight is unremarkable, the status should remain outpatient without the addition of observation hours.
In the April 7, 2000 Outpatient Prospective Payment System (OPPS) Final Rule (65 FR 18455), in explaining the criteria for selection of procedures for the Inpatient-Only List, CMS noted that “the inpatient list specifies those services that are only paid when provided in an inpatient setting because of the nature of the procedure, the need for at least 24 hours of postoperative recovery time or monitoring before the patient can be safely discharged, or the underlying physical condition of the patient.” Thus, one of the criteria that distinguishes inpatient surgery from outpatient surgery is an expected length of stay of up to 24 hours for outpatient procedures and greater than 24 hours for inpatient. This offers additional evidence indicating that there is no need to change patient status for an overnight stay following uncomplicated outpatient surgery when the stay is expected to be less than 24 hours. Notice that in both cases, whether discussing the expected length of stay for a patient having outpatient surgery or one having an inpatient procedure, it’s the physician’s expectation at the time of admission that determines the proper level of care, not the actual length of stay, as viewed in retrospect.
In the 2018 OPPS Final Rule, CMS refers back to their 2012 OPPS/ASC Final Rule for discussion on how they identify procedures that are “typically provided only in an inpatient setting” and therefore are on the Inpatient-Only List. But, in true CMS fashion, looking at the 2012 Final Rule, you’ll find it references the April 2000 OPPS Final Rule. This is the same discussion Dr. Meyerson references about, “the need for at least 24 hours of postoperative recovery time or monitoring before the patient can be safely discharged.” But it’s important to recognize this is not a direction to place a procedural patient who has an anticipated need for 24 hours of monitored recovery into inpatient status.
So if the patient can stay overnight in a hospital bed following outpatient tests or surgery without observation, when would observation be appropriate? WPS Medicare (LCD L32222) explained that when a patient has a significant adverse reaction (beyond the usual and expected response) as a result of the test that requires further monitoring, outpatient observation or inpatient hospital services may be reasonable and necessary.
Outpatient with observation services? Yes. Inpatient? Only if the patient ends up requiring a second midnight of care, or if you want to test your luck with the vague concept of the physician judgment exception added by CMS into the Two-Midnight Rule on Jan. 1, 2016. (See Dr. Ronald Hirsch’s article at https://www.racmonitor.com/the-new-short-stay-exception-read-before-using to learn more.)
TMF Health Quality Institute, the Texas Medicare QIO, in its Medicare Outpatient Observation Physician Guidelines Q&A, answered the question, “Can a same-day surgery patient with no postoperative complications be admitted to observation?” TMF responded “No. There must be medical necessity of observation services documented in the medical record. Observation is not to be used as a substitute for recovery room services.” Another question asked, “Can a patient be placed in observation status prior to outpatient surgery?” TMF’s answer: “No. The need for observation care should be determined by the patient’s condition during the postoperative recovery period, not prior to surgery.”
TMF further described other situations in which observation would not be appropriate for surgical patients, such as:
Routine stays following late surgery;
Outpatient therapy/procedures (unless there is documentation that the patient’s condition is unstable);
Normal postoperative recovery time following surgery;
Stays for the convenience of the patient, family, or doctor; and
Stays prior to an outpatient surgery procedure.
TMF who? TMF Health Quality Institute evolved into a different kind of QIO since the spring of 2013, when Dr. Meyerson’s original article was published, as currently, the only Beneficiary and Family Centered Care (BFCC) QIOs in action are Livanta and Kepro when it comes to hospitals. The points given above still ring true, though, when it comes to situations that would not be appropriate for observation hours.
TMF even supplied a list of typical postoperative problems that warrant observation:
Persistent nausea/vomiting;
Fluid/electrolyte imbalance;
Uncontrolled pain;
Dysrhythmias;
Excessive/uncontrolled bleeding;
Psychotic behavior;
Unstable level of consciousness; and
Deficit in mobility/coordination.
This is helpful, too, and still applicable. Remember that anything that requires additional assessment, care, or treatment beyond routine recovery means an observation order should be placed by the provider. The list above only scratches the surface of reasons why a patient might be appropriate for observation services.
So, what should a surgeon or proceduralist do if no adverse event has occurred, but the physician wants to extend monitoring because the patient is at risk for complications or may not recover as expected due to age, frailty, or comorbidities? The proper approach would be to use overnight recovery in an outpatient bed. There would be no need to order observation because an adverse event did not occur; the physician may order observation only after such an event, and the medical record must indicate clearly the reason that observation was medically necessary. A surgeon concerned about the risk of complications would order extended recovery, monitor the patient overnight (as an outpatient in a bed), and either release the patient the next day or order observation (or admission) if a complication does occur.
This paragraph still rings true, but I’d like to point out that supporting the term “extended recovery” can be a slippery slope. Many institutions used this designator interchangeably with “observation” or “23-hour observation” back in the days when needing 24 hours or more of hospitalization equaled inpatient status. I have found that sticking with “inpatient,” “observation,” and “outpatient in a bed” makes things much clearer.
It’s ironic, and somewhat illogical, that a patient may be admitted to the hospital as an inpatient prior to surgery for what ordinarily would be an outpatient procedure if the surgeon is concerned about a high risk of complications due to the patient’s clinical condition or past history, but the surgeon would not order observation based on a similar risk assessment after the operation or procedure.
This is exactly why, almost five years later, when the 2018 OPPS Final Rule came out about including direction about total knee arthroplasties, which were taken off the Inpatient-Only List, there was much angst and gnashing of teeth.
Some surgeons are uncomfortable placing a patient in an outpatient bed overnight following surgery without ordering observation. They should be reassured that this is not a quality or safety issue. The same monitoring and treatment may be ordered for a patient in overnight recovery as for a similar patient who has observation services ordered. Some also are concerned about the financial implications, and feel that if they order observation, “at least the hospital gets paid.” Unfortunately, this is not always the case. Contrary to CMS policy, which provides for payment to the hospital for observation services for a patient placed into observation from the ED or from a physician’s office, “if a hospital provides a service with status indicator ‘T’ on the same date of service, or one day earlier than the date of service associated with HCPCS code G0378 (used to denote observation hours), the composite APC 8003 (used to bill the observation stay for patients placed into observation from the ED) would not apply … HCPCS code G0378 will continue to be assigned status indicator ‘N,’ signifying that its payment is always packaged.” In other words, if a patient has an outpatient procedure (status indicator “T” or “J1” on CMS Addendum B), the hospital does not receive any additional payment for observation. It is “packaged” into the Ambulatory Payment Classification (APC) payment for the procedure whether observation is ordered or not. (OPPS Final Rule, Nov. 1, 2007, CMS-1392-FC.)
Today, instead of APC 8003, we have C-APC 8011 to bill observation stays. However they are still separated from an outpatient procedure with status indicator “T” or “J1” on CMS Addendum B, and there is no additional payment given to the hospital for the observation services. This does not mean there is no reason to pursue an order for observation services, when appropriate. Remember that for quality tracking purposes, including assessment of length of stay, it’s important to identify which patients followed a regular and routine recovery pathway, and which did not. Also, while Fee-for-Service Medicare does not provide additional payment for observation services in these cases, your other payors likely do.
Notice that the TMF list of situations in which observation would not be appropriate includes “stays prior to an outpatient surgery procedure.” It adds that observation cannot be used for a prep of any kind, including, for example, preoperative hydration or cardiac assessment, bowel prep, or “renal protection protocol.” Nor can observation be based on time spent in recovery. Observation is properly used only if an intra- or post-op procedure complication actually occurs.
I’d like to interject here with an example of a rare instance where pre-hospitalization for observation services before a procedure would be justified. Mind you, this is the only case I saw in almost nine years of serving as a health system physician advisor, but it demonstrates that it is a possibility. The patient, a brittle Type 1 diabetic, was scheduled for a colonoscopy. The gastroenterologist was concerned because when the patient was prepped at home for the same procedure just a year before, she developed profound hypoglycemia, to the extent that she required emergency care and subsequent hospitalization for stabilization. In this case, the patient truly required pre-hospitalization, not simply to carry out the GI prep, but also to administer IV fluids with dextrose and closely monitor her blood glucose levels for active treatment, either with adjustments to the fluids or adjustments to her insulin administration.
If surgery or a procedure interrupts observation and the patient returns to the observation bed for continued evaluation or short-term treatment, and there is still a question of whether the patient will have to be admitted, observation would continue – but the time the patient was under “active monitoring” in the operative suite (including routine recovery in the post-anesthesia care unit) would be carved out for billing purposes.
This remains true.
So far, Recovery Audit Contractor (RAC) auditors have not paid a lot of attention to the use of observation. With respect to postoperative observation, since there is no additional payment, there would be no incentive for an auditor paid on a contingency fee basis to bother auditing these records. However, there is reason to be concerned about proper use of observation for surgical patients, since Medicare requires accurate billing even if there is no payment rendered. In its 2012 and 2013 Work Plans, the U.S. Department of Health and Human Services (HHS) Office of Inspector General (OIG) outlines a focus on “observation services during outpatient visits.”
“We will review Medicare payments for observation services provided by hospital outpatient departments to assess the appropriateness of the services and their effect on Medicare beneficiaries’ out-of-pocket expenses for healthcare services,” the precise language reads. So even though there is no significant effect on Medicare beneficiaries’ out-of-pocket expenses for postoperative observation, if the OIG investigates a hospital’s use of observation due to an excessive number of such claims filed as compared to peers, the hospital could face a compliance challenge if the review reveals inappropriate and/or excessive use of observation.
I did not investigate the outcome of the OIG Work Plans in 2012 and 2013 mentioned above. Looking at the active Work-Plan items on the OIG website involving “observation,” there is only one involving hospital care, dated November 2016 and titled Medicare Payments for Transitional Care Management. However, this involves care management services provided to patients moving from a hospital, partial hospital, or skilled nursing facility to the community setting, and not specifically observation services provided in the hospital setting.
Considering the limited circumstances under which postoperative observation is appropriate, and the lack of reimbursement for the service, hospitals would be wise to monitor the use of observation among these patients and ensure that when observation is billed, there are documented postoperative complications – and that observation is not used for preoperative preparation or for routine postoperative recovery.
Agreed! If your hospital’s surgeons and proceduralists continue to place patients into outpatient status with observation services for routine postoperative care, that’s a situation that needs to be addressed. Conversely, education is also imperative to ensure justified observation hours are captured and billed. From your providers to the bedside nurses to the case and utilization managers, do they know when an observation order should be entered? Make it a point to ask around…you might be surprised what you find.

How Do We Code Outpatient Surgeries-Turned-Hospitalizations?
In essence, you are telling the story of the surgery and what happened during recovery in codes. You need the provider to document so you understand the course of events and whether there was a complication or not.
By Erica E. Remer, MD, CCDS
Recently I wrote about when surgery should be performed as an inpatient, when it can be outpatient, and how to utilize observation services in the context of surgical procedures. Now, I want to tackle how to document and code such encounters compliantly. I’d like to thank Colleen Ejak, Kathy Murchland, Damon Schmelzle, and ICD10monitor’s Laurie Johnson and Patty Chua for their sage advice.
Let’s use as our example a Medicare patient with chronic cholecystitis who has a laparoscopic cholecystectomy. The procedure is not on the Inpatient-Only (IPO) List, so, barring extenuating circumstances like having high-risk comorbidities, it will be done as an outpatient. For right now, let’s stipulate that it is being done in a hospital-based outpatient surgery department.
Undergoing this procedure as an outpatient surgery, the patient is expected to be in the recovery room for a limited amount of time and then discharged to home. The first-listed diagnosis is K81.1, Chronic cholecystitis, and the procedure is billed as with Current Procedural Terminology (CPT®) Code 47562, Laparoscopy, surgical; cholecystectomy.
Let’s say that the surgery was scheduled as the last procedure of the day, and ended up getting bumped so late that the surgeon takes pity on the patient and says, “Let’s keep you overnight to watch you.” Without any complications or unusual issues with recovery, an overnight stay for convenience is just an extended recovery or overnight/outpatient in a bed. These do not constitute observation services. Also, an observation stay cannot be scheduled in advance. Dr. Ronald Hirsch’s saying is that if your provider is scheduling observation prior to the procedure, they are scheduling a complication – and maybe you should find someone else to do the surgery.
Now, say our newly gallbladder-less friend begins vomiting from the anesthesia and just can’t stop. They now have the complication of intractable vomiting. We have every hope that this will stop within about 24 hours, so placing the patient in outpatient status for observation services (OBS) is reasonable. ICD-10-CM Guidelines for Coding and Reporting, IV.A.2., states that the reason for the surgery is the first reported diagnosis (it is the reason for the encounter), followed by codes for the complications as secondary diagnoses.
Therefore, her first-listed diagnosis (the outpatient correlates to the principal diagnosis (PDx) for an inpatient admission) is K81.1, Chronic cholecystitis. But what would the secondary diagnosis/diagnoses be?
Before we tackle the secondary diagnoses, let’s address the procedure. Since the procedure and the observation stay are in the same hospital, the encounters are combined (for the technical component). The 47562, Laparoscopic cholecystectomy, would also be coded on the outpatient claim with observation hours. But it does not get coded if the entities were not related; e.g., outpatient surgery in an ambulatory surgical center (ASC) not affiliated with the hospital to which the patient was transferred (I’ll get to this scenario in a moment).
The issue is vomiting, so a secondary diagnosis would be R11.10, Vomiting, unspecified. But does that tell the whole story? Especially if the procedure is not coded as in the ASC/observation case, how can we tell that the patient had an operation?
If the procedure were an appendectomy, you would use K91.0, Vomiting following gastrointestinal surgery. This is a combination code – it informs us that there is vomiting and the circumstances that elicited the vomiting (that it is post-surgical). Cholecystectomy isn’t gastrointestinal surgery – it is on the biliary tract. It is in the digestive system, but it isn’t gastrointestinal. The fact that the gastrointestinal Procedure Coding System falls into 0D and gallbladder procedures fall into 0F supports this position.
I posit that ICD-10-CM code K91.89 and other postprocedural complications and disorders of the digestive system should be assigned. R11.10 would be an “additional code, if applicable, to further specify disorder.” K91.89 gives that piece of information that the patient underwent a surgical procedure, and the issue is a postprocedural complication. R11.10 indicates what the postprocedural complication was.
An aside – K91.5, Post-cholecystectomy syndrome (PCS), is a condition in which a patient undergoes a cholecystectomy and the symptoms that elicited the surgical intervention persist or recur – or new symptoms normally attributed to the gallbladder arise. Right upper-quadrant abdominal pain and dyspepsia are common. It is considered early if it occurs in the postoperative period, but it can manifest after months or years in the late variant. If the provider documented “post-cholecystectomy syndrome” for our exemplar, you would pick this code up. If they document “intractable vomiting” or “persistent vomiting post-anesthesia,” PCS would not be appropriate.
The next scenario is that the same outpatient surgery patient placed in observation with intractable vomiting gets so dehydrated that they ends up in renal failure; in this case, it is clear they are going to cross a second midnight, so the provider converts them to inpatient. According to II. I. 2., “When a patient is admitted to observation to monitor a condition (or complication) that develops following outpatient surgery, and then is subsequently admitted as an inpatient of the same hospital, hospitals should apply the Uniform Hospital Discharge Data Set (UHDDS) definition of PDx as ‘that condition established after study to be chiefly responsible for occasioning the admission of the patient to the hospital for care.’”
The acute kidney injury (AKI) is the reason they are being admitted, so you would think N17.9, Acute kidney failure, unspecified, could be the PDx. However, I would still say that there is a direct line from the postoperative complication (vomiting) to the dehydration causing AKI, and therefore, K91.89 is still the PDx. E86.0, Dehydration, N17.9, and R11.10 would be secondary diagnoses.
The other twist is that the procedure gets converted into ICD-10-PCS. It will likely drive the Diagnosis-Related Group (DRG) and is included because it is part of the episode of care, according to the three-day payment window rule.
We have to digress for a moment again. This surgery was done in a hospital-based outpatient setting. For Medicare patients, the technical component of all outpatient diagnostic services and therapeutic services considered related, within the three days preceding, get bundled into an inpatient admission. This is called the three-day payment window rule or policy and applies to entities wholly owned or wholly operated by the hospital. This may encompass more than 72 hours because it is according to the calendar day.
There is an exclusion if the hospital and other Part B entity are both owned by a third party, such as a comprehensive healthcare system. It also doesn’t apply if the entities are not related in any way. Psychiatric hospitals and units, inpatient rehabilitation hospitals and units, long-term care hospitals, children’s hospitals, and cancer hospitals have a one-day payment window.
The final setup is directly admitting a patient from outpatient surgery. Let’s use a different example this time because there are three scenarios to discuss. I’m choosing acute appendicitis seen in the emergency department. If the patient is sick and/or has significant comorbidities and risk, they may get admitted inpatient prior to the surgery, even though appendectomy is not on the IPO List. However, sometimes, the surgeon takes the patient to the operating suite intending for it to be an outpatient procedure, and then has to pivot after surgery.
Scenario 1: The patient has a complication after or during surgery. Let’s pick accidental puncture and laceration of the bowel with contents spillage. K91.71, Accidental puncture and laceration of a digestive system organ or structure during a digestive system procedure is the PDx, as per II. J. Admission from Outpatient Surgery. If the reason for the inpatient admission is a complication, that is assigned as the PDx. If the complication is from T80-T88 or is too generic and lacks specificity, an additional code for the specific complication is indicated. The condition that elicited the procedure is a secondary diagnosis. The procedure is included on the claim in the ICD-10-PCS form.
Scenario 2: During the procedure, it was determined that the appendicitis was more complicated than the imaging suggested. There was perforation or a poorly visualized abscess, and the surgeon realized that it was going to take several days of antibiotics and monitoring to ensure a good outcome. They write admission orders and convert the outpatient surgery to an inpatient admission. The PDx is the reason for the operation, found in K35.-, Acute appendicitis, with specificity (generalized or localized peritonitis, abscess, perforation, and/or gangrene). II.J. stipulates: “if no complication, or other condition, is documented as the reason for the inpatient admission, assign the reason for the outpatient surgery as the PDx.”
If the hospital owns the outpatient surgical center (or ASC, for an appropriate procedure), the procedure would be coded. But if the hospital doesn’t own it, how do you convey that the patient is postoperative? Could you use Z90.49, Acquired absence of other specified parts of the digestive tract, to signify that the patient had undergone an appendectomy? This type of Z code, or status code, indicates “that a patient has the sequelae or residual of a past disease or condition” [I.C.21.3)]. This isn’t a “past disease or condition” yet. Z90.49 (when relevant) will be used in the future, but it is not appropriate until the patient has completely healed.
What I am going to say now may be controversial. I think you would use Z48.815, Encounter for surgical aftercare following surgery on the digestive system. This conveys that the patient is still in the recovery phase after a procedure. II.21.c.7 instructs that this type of code be used “when the patient requires continued care during the healing or recovery phase.” The American Hospital Association’s ICD-10-CM and -PCS Coding Handbook says: that aftercare codes “can be used occasionally as additional codes when aftercare is provided during an encounter for treatment of an unrelated condition but no applicable diagnosis code is available. Aftercare codes should be used in conjunction with any other aftercare or diagnosis code(s) to provide better detail on the specifics of an aftercare visit…” We have the details of the underlying condition that caused the surgery, but we don’t, as yet, have a code indicating that surgery was done for that condition and the patient is in the recovery phase.
If the hospital owned both entities, the payment episode was continuous, and the procedure is enfolded into the encounter. If the hospital does not, then the payment episode is interrupted, and Z48.815 could communicate that the patient was post-surgical. Especially now that we treat some acute appendicitis with antibiotics instead of cold, hard steel, we definitely need a mechanism to signal that the patient has been operated upon.Scenario 3: The patient has a comorbidity that occasionally flares up, and it does so in the recovery room or has a new condition not felt to be directly due to the surgery, per se. Perhaps the provider explicitly links it to something other than the surgery (e.g., acute-on-chronic hypercapnic respiratory failure due to exacerbation of COPD). Don’t get confused like clinicians do – just because it occurs in the postoperative period doesn’t make it cause-and-effect, a requisite for recognizing a complication for ICD-10-CM.
As per II.J., “If the reason for the inpatient admission is another condition unrelated to the surgery, assign the unrelated condition as the PDx.” J44.1, Chronic obstructive pulmonary disease with (acute) exacerbation, would be the PDx; J96.22, Acute and chronic respiratory failure with hypercapnia and K35.30, Acute appendicitis with localized peritonitis without perforation or gangrene, would be secondary diagnoses, and 0DTJ4ZZ, Resection of Appendix, Percutaneous Endoscopic Approach, would be the principal procedure.
If the coder is unsure, they may need to query. For instance, a query to ascertain whether the provider believes the new-onset atrial fibrillation is a postprocedural complication or unrelated may be necessary (i.e., is it I97.191, Other postprocedural cardiac functional disturbances following other surgery with I48.91, Unspecified atrial fibrillation, or just I48.91?).
Along those lines, an unrelated medical condition arising in recovery resulting in the provision of observation services would be first-listed, the condition causing the surgery would be a secondary diagnosis, and the procedure would be coded only if the observation site was owned by the same hospital as the outpatient surgical center. Again, I endorse Z48.815, Encounter for surgical aftercare following surgery on the digestive system to indicate the postoperative status if the surgical site was not owned by the hospital providing the observation services. There is a whole set of surgical aftercare codes available in Z48.8-.
Bottom line, here’s my flow chart:
Intraoperative or postprocedural complication
Observation stay
Reason for surgery is the first-listed diagnosis
Complication code secondary
Additional code describing complication, if applicable
(Other comorbidities’ secondary diagnoses, if applicable)
Hospital owns both outpatient surgery center and observation = CPT code
Independent outpatient/ASC and hospital observation = No procedure code. The fact that the patient is post-op is inherent in the complication code.
Observation to inpatient conversion
Reason for conversion to inpatient is PDx (likely will be the complication)
Reason for surgery is secondary diagnosis
Additional code describing complication, if applicable
(Other comorbidities’ secondary diagnoses, if applicable)
Hospital owns both outpatient surgery center and observation = ICD-10-PCS code
Independent outpatient/ASC and hospital observation = No procedure code. The fact that the patient is post-op is inherent in the complication code.
Inpatient admission directly
Complication code is PDx
Reason for surgery is secondary diagnosis
Additional code describing complication, if applicable
(Other comorbidities secondary diagnoses, if applicable)
Hospital owns outpatient surgery center = ICD-10-PCS code
Independent outpatient/ASC and hospital observation = No procedure code. The fact that the patient is post-op is inherent in the complication code.
Needs further hospital-level care following procedure without complication
Observation stay
Reason for surgery is first-listed diagnosis
Other comorbidities secondary diagnoses, if applicable
Hospital owns both outpatient surgery center and observation = CPT code
Independent outpatient/ASC and hospital observation = No procedure code and no complication code. Use Z48.815, Encounter for surgical aftercare following surgery on the digestive system, as additional diagnosis.
Observation to inpatient conversion
Reason for conversion to inpatient is PDx (according to UHDDS – probably the reason for surgery)
Reason for surgery is either primary or secondary diagnosis
Other comorbidities’ secondary diagnoses, if applicable
Hospital owns both outpatient surgery center and observation = ICD-10-PCS code
Independent outpatient/ASC and hospital observation = No procedure code and no complication code. Use Z48.815, Encounter for surgical aftercare following surgery on the digestive system, as additional diagnosis.
IP admission
PDx according to UHDDS (probably the reason for surgery)
Reason for surgery is either primary or secondary diagnosis
Other comorbidities’ secondary diagnoses, if applicable
Hospital owns outpatient surgery center = ICD-10-PCS code
Independent outpatient/ASC and hospital observation = No procedure code and no complication code. Use Z48.815, Encounter for surgical aftercare following surgery on the digestive system, as additional diagnosis.
Unrelated medical condition arises that is not a postoperative complication and requires observation or inpatient (if the documentation is not clear, may need a query to determine if complication or unrelated)
Observation stay
Unrelated medical condition causing observation is first-listed diagnosis
Reason for surgery is secondary diagnosis
Other comorbidities’ secondary diagnoses, if applicable
Hospital owns both outpatient surgery center and observation = CPT code
Independent outpatient/ASC and hospital observation = No procedure code and no observation code. Use Z48.815, Encounter for surgical aftercare following surgery on the digestive system, as additional diagnosis.
Observation to inpatient conversion
Reason for conversion to inpatient is PDx (according to UHDDS – in this case, it is likely the unrelated medical condition)
Reason for surgery is secondary diagnosis
Other comorbidities’ secondary diagnoses, if applicable
Hospital owns both outpatient surgery center and observation = ICD-10-PCS code
Independent outpatient/ASC and hospital observation = No procedure code and no complication code. Use Z48.815, Encounter for surgical aftercare following surgery on the digestive system, as additional diagnosis.
IP admission
Unrelated medical condition is PDx according to UHDDS
Reason for surgery is secondary diagnosis
Other comorbidities’ secondary diagnoses, if applicable
Hospital owns outpatient surgery center = ICD-10-PCS code
Independent outpatient/ASC and hospital observation = No procedure code and no complication code. Use Z48.815, Encounter for surgical aftercare following surgery on the digestive system, as additional diagnosis.
This was a fascinating thought exercise! In essence, you are telling the story of the surgery and what happened during recovery in codes. You need the provider to document so you understand the course of events and whether there was a complication or not. As far as how it gets put on the claims and gets billed, or what condition codes or modifiers you use, you need a real person from revenue cycle to counsel you on that! I hope you found this as interesting as I did. Let me know if you agree, or if it changes your practice (icd10md@outlook.com).

Understanding the U.S. Playbook to Address the Social Determinants of Health
The Biden Administration has released a new playbook addressing three “pillars” of emphasis related to the social determinants of health (SDoH), from the Domestic Policy Council’s Office of Science and Technology Policy.
By Tiffany Ferguson, LMSW, CMAC, ACM
The Biden Administration has released a new playbook addressing three “pillars” of emphasis related to the social determinants of health (SDoH), from the Domestic Policy Council’s Office of Science and Technology Policy. While acknowledging the extensive coverage of the evidence and the significance of the SDoH across various media outlets, this review aims to delve into the specific strategies and allocation of resources by the White House to support SDoH initiatives and advance health equity.
Pillar 1: Data Expansion
The first pillar is centered on expanding data acquisition and sharing. The Administration plans to achieve this by fostering enhanced interagency collaboration and standardization of social data collection methods. Key efforts include the establishment of a centralized federal data working coalition, overseen by the Office of the Federal Chief Information Officer within the Office of Management and Budget (OMB). The overarching objective is to adopt a “whole-of-government” approach toward SDoH data collection and management. This involves aligning regulations and leveraging purchasing power in both public and private sectors for health information technology.
Moreover, measures will be taken to protect the exchange of individuals’ sensitive health information across federal agencies, with an expectation of expanded privacy guidelines by the U.S. Department of Health and Human Services (HHS). Notably, the playbook also highlights the need to bridge connection gaps, emphasizing closed-loop referrals. A substantial focus is also dedicated to the “Enterprise-Wide Veteran Social Determinants of Health Framework Integrated Project Team” to address veterans’ SDoH-related needs.
Pillar 2: Flexible Funding for Social Needs
The second pillar emphasizes the allocation of flexible funding for SDoH investments within Medicaid. This involves providing states with guidance on the use of lieu of services and settings (ILOS) to enable managed Medicaid programs to offer optional alternatives to state-plan covered services.
The playbook provides a recap of HCPCS code G0136, which provides reimbursement for SDoH risk assessment. Furthermore, the funding expansion aims to bolster grant eligibility and enhance nutrition support programs such as the Supplemental Nutrition Assistance Program (SNAP), Women, Infants, & Children (WIC), and school-based meals.
Pillar 3: Backbone Organizations
The third pillar focuses on backbone organizations, which act as facilitators managing community-based partnerships across sectors like healthcare, social services, public health, and economic development. The playbook emphasizes training and technical assistance for community care hubs through the National Learning Community.
It also proposes new funding opportunities for growth and expansion, with a specific emphasis on supporting families, early childhood support, and at-risk neighborhoods. Additionally, it expresses a keen interest in enhancing legal services for patients at health centers and advocates for greater attention to environmental justice needs impacting health outcomes.
From a review of the playbook, it is clear that some of these projects have already been started, while others are still yet to be fleshed out for funding allocation; the question remains regarding how this will trickle down to healthcare organizations and communities. As of today, the message focuses on the importance of collecting meaningful SDoH data at both the patient level and macro levels, across agency sectors, for community impact, with intentions for future growth.
Healthcare funding and efforts will continue to focus on expanding healthcare coverage in non-traditional settings, such as street medicine, and bringing non-typical services into the health sector, such as housing assistance, meal delivery, and legal support services. The playbook concludes with an envisioned future “where health and social circumstances can be addressed holistically and equitably.”